
.png)

Mental Health Concerns
Claustrophobic Meaning, Symptoms & Treatment: Complete Guide to Claustrophobia

.png)
Written by
Aarohi Parakh,
Psychologist and Content Writer

Reviewed by
Sanjana Sivaram,
Psychologist and Clinical Content Head






Introduction
It is 8:47 on a Monday morning. Arya, a 34-year-old software engineer from Mumbai, is standing on Platform 4 of the Andheri, Mumbai Local. The train arrives packed to the doors. She watches a dozen people squeeze in. She steps forward. Her heart immediately begins to race. Her chest tightens. The doors feel like walls closing in on her. She steps back. She will be late for the third time this month. She does not have words for what just happened. She only knows that she cannot get on that train.
If you recognise something of yourself or someone you know in Arya's experience, you are not alone. And what she experienced has a name. This guide will breakdown on what claustrophobia means, its symptoms, Magnetic Resonance Imaging (MRI) tips for people who are claustrophobic, and effective treatment options.
What Does Claustrophobic Mean? Meaning & Definition
"Claustrophobic" describes a person who has claustrophobia — an intense, irrational fear of enclosed or confined spaces. Claustrophobia is classified as a specific phobia under anxiety disorders in the DSM-5 (Diagnostic and Statistical Manual of Mental Disorders, 5th Edition), the gold-standard diagnostic guide used by mental health professionals worldwide.
In everyday usage, people sometimes say "I'm claustrophobic" loosely, to mean they feel a bit uncomfortable in crowded or cramped spaces. But in the clinical sense, being claustrophobic means experiencing severe anxiety, panic symptoms, and an overwhelming urge to escape whenever you are in a small or confined environment (claustro means closed).
Claustrophobic Meaning in Indian Languages
For readers across India, here is the claustrophobic meaning in your language:
- Hindi (claustrophobic meaning in Hindi):
संकुचित स्थानों का डर / बंद जगह से डर लगना (bund jagah se dar lagna)
- Bengali (claustrophobic meaning in Bengali):
আবদ্ধ স্থানের ভয় (aboddho sthaner bhoy)
- Telugu (claustrophobic meaning in Telugu):
మూసిన స్థలాల భయం (moosina sthalala bhayam)
- Marathi (claustrophobic meaning in Marathi):
बंद जागेची भीती (band jagechi bhiti)
- Malayalam (claustrophobic meaning in Malayalam):
അടച്ചിട്ട ഇടങ്ങളോടുള്ള ഭയം (adachitta idangalodulla bhayam)
Common triggers for Claustrophobia comprise:
- Tunnels
- Elevators
- Public restrooms
- Trains
- Airplanes
- Small cars
- Caves
- Revolving doors
- MRI imaging machine
- Cellars
- Miniature rooms that don’t have windows or have windows that can’t be opened.
- Thoughts about being in a confined space.
Is Fear of Elevators the Same as Claustrophobia?
Readers sometimes search for "fear of elevators (not claustrophobic)", wondering if elevator fear is something distinct. In most cases, a specific and intense fear of lifts is a form of claustrophobia because the core trigger is the enclosed, inescapable nature of lifts. In rare cases, elevator fear can stem from a fear of mechanical failure (a safety fear) rather than from confinement. If lifts are your primary trigger and other enclosed spaces do not bother you, it is still worth speaking with a clinical psychologist to identify what is actually driving the anxiety.
Claustrophobia vs Feeling Uncomfortable in Small Spaces: What Is the Difference?
Feeling a little uneasy in a very cramped space is a common human response. If you have ever squeezed into a crowded lift and felt relief when the doors opened, that reflects how our mind and body react to limited space. Enclosed environments can sometimes pose real risks, so a degree of caution makes biological sense.
Claustrophobia, however, is clinically different. It crosses the threshold from discomfort into disorder when:
- The fear is disproportionate to the actual danger of the situation
- Exposure to the enclosed space almost always triggers immediate and intense anxiety or panic
- The person actively avoids enclosed spaces in ways that disrupt daily life
- The fear has persisted for six months or more
- The anxiety or avoidance causes significant distress or functional impairment
These are the diagnostic criteria outlined in the DSM-5 by the American Psychiatric Association, and they distinguish a clinical phobia from ordinary discomfort.

In everyday Indian life, many people experience claustrophobia in practical situations. People with claustrophobia might climb 12 flights of stairs rather than take the lift in a high-rise office building. They might travel by road for hours to avoid the Mumbai local or Delhi Metro during peak hours. They might delay or outright refuse an MRI scan that their doctor has recommended, sometimes at the cost of serious health consequences.
Claustrophobia Symptoms: What Happens During an Episode?
When a claustrophobic person enters a triggering space, the brain's threat-detection system (the amygdala) fires as though there is a genuine danger. The body triggers a full fight-or-flight response. From the inside, this is what it may feel like:
Claustrophobia Symptoms: At a Glance
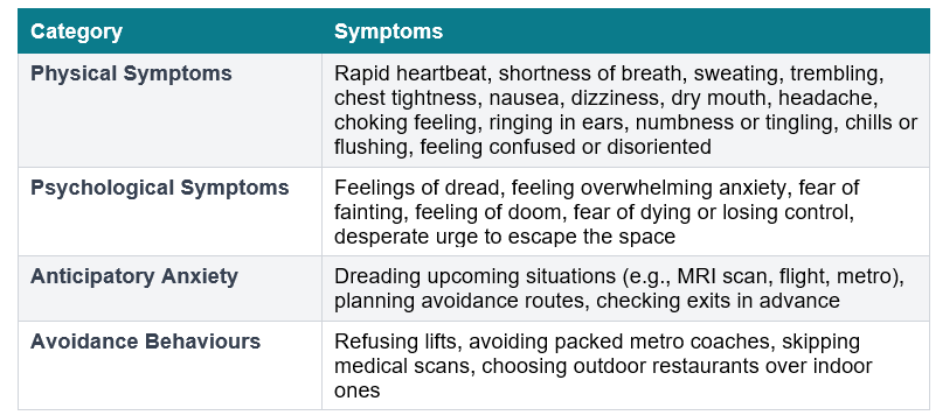
The panic typically peaks within ten minutes and begins to subside once the person escapes the enclosed space. However, for many people, the anticipatory anxiety, or the dread that builds before they even reach the trigger, can be just as exhausting as the episode itself.
Common Claustrophobia Triggers in India
- Crowded public transport during peak hours
- MRI and CT scan tunnels at diagnostic centres
- Old, small lifts in residential buildings and government offices
- Underground corridors or basements of malls and hospitals
- Small temple sanctum sanctorums during festivals
- Crowded bazaars or narrow market lanes in old city areas
- Airplanes during turbulence or when seated in the middle rows

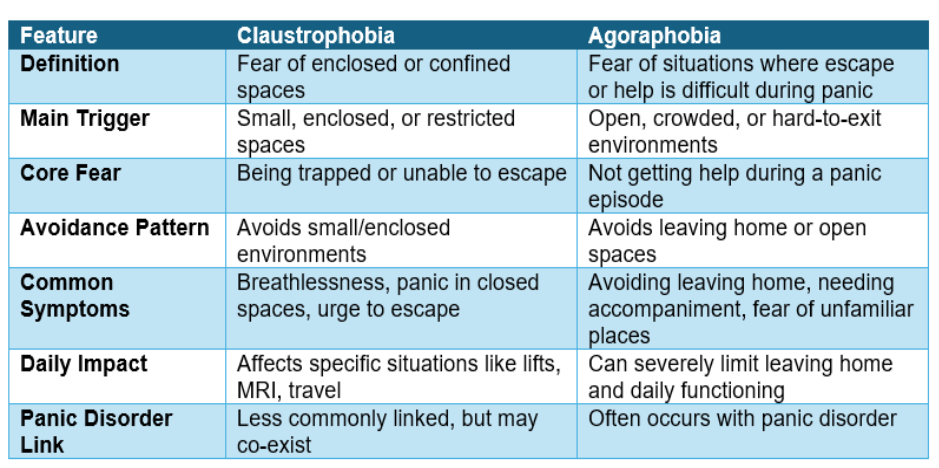
Claustrophobia vs Agoraphobia: Opposite Fears, Similar Mechanisms
While both conditions are subtypes of anxiety disorders, they can manifest and impact people in distinctly different ways.
People can often get confused about agoraphobia because of the similarity in their symptoms. Both of these phobias are characterized by intense fear, avoidance of anxiety-causing situations, and physical symptoms such as breathlessness, dizziness, racing heart, etc. The table below clarifies the distinction:
Claustrophobia & MRI Scans: What to Do If You Are Claustrophobic
For many individuals with claustrophobia, being referred for an MRI scan triggers enormous anxiety, even before the appointment. This is understandable. A standard closed MRI machine places you inside a narrow cylindrical bore of about 60 centimetres in diameter, requires you to remain still for around 15 to 45 minutes, and produces repeated loud knocking or banging sounds. For someone with claustrophobia, this environment can feel particularly challenging.
The important thing to know is this: you do not have to struggle your way through it, nor do you have to skip the scan entirely. There are real, practical solutions.
💡Medical Note: MRI avoidance due to claustrophobia is a documented public health issue in India. Delayed diagnosis of neurological conditions, joint problems, and cancers due to refused scans is a serious and preventable outcome. Always inform your radiologist about your claustrophobia before your appointment.
Options for Claustrophobic Patients Needing an MRI
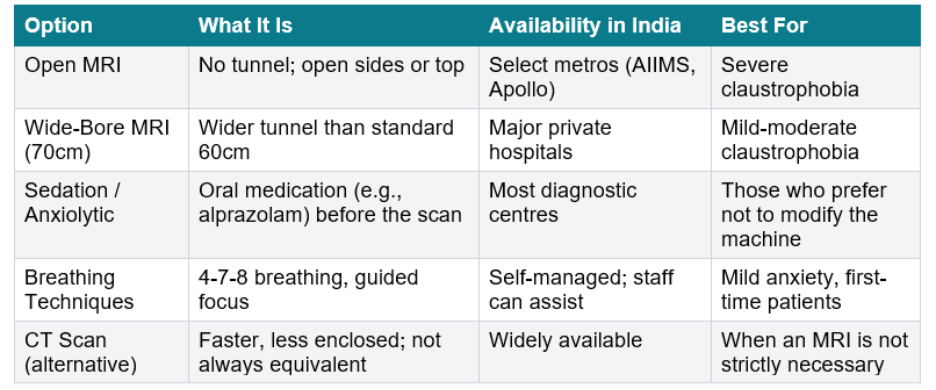
When Is an MRI Truly Necessary vs Replaceable?
A CT scan is faster (often 10-15 minutes) and involves a much shorter, shallower tunnel. For some conditions, a CT scan provides equivalent or sufficient diagnostic information. However, in some cases such as neurological disorders, soft tissue injuries, or certain cancers, an MRI may be specifically recommended because it provides more detailed imaging than other scans. n such situations, it’s best to discuss options with your referring doctor before assuming alternatives will be suitable for your needs.
💡Pro-Tip: When booking your MRI, ask specifically: (1) Does this facility have a wide-bore (70cm) machine? (2) Can I have a radiographer in the room with me? (3) Can I listen to music through headphones during the scan? These three questions alone can dramatically reduce anxiety during the procedure.
What Causes Claustrophobia? Origins & Risk Factors
Claustrophobia does not arise suddenly. Like most specific phobias, it develops from a mix of experiences, learned responses, biological factors, and genetic factors. Understanding these origins can reduce the self-blame often associated with it.
Key Causes and Risk Factors (With Examples)
- Direct Conditioning
A distressing experience involving confinement can create a lasting fear response.
Example: Getting stuck in a lift for 20 minutes during a power cut or being accidentally locked in a small room as a child.
- Vicarious Learning
Seeing someone else panic in an enclosed space can shape your own fear response.
Example: Watching a family member panic during an MRI or seeing someone struggle in a crowded train compartment.
- Evolutionary Basis
Humans are wired to be cautious in environments where escape is limited.
Example: Feeling uneasy in a tightly packed elevator or a windowless basement with no clear exit.
- Genetic Predisposition
A family tendency toward anxiety or phobias can increase vulnerability.
Example: Growing up with a parent who avoids lifts or crowded spaces and gradually developing similar fears.
- Brain Mechanisms (Amygdala Response)
The brain may overreact to perceived threats, even when there is no real danger.
Example: Feeling a sudden surge of panic while entering an MRI machine or even when imagining being in a confined space.
- Trauma-Linked Factors (India-Specific Context)
Real-life emergencies or disasters can imprint strong fear associations.
Example: Being trapped during a building collapse, stuck in floodwaters, or caught in a crowded situation with no easy escape.
In such cases, claustrophobia may overlap with post-traumatic stress, making it important to address both the trauma and the phobia for effective recovery.
Neuroscience Insight
Claustrophobia is linked to increased activity in the brain’s fear circuit. Studies show that individuals with claustrophobia exhibit heightened amygdala activation even when exposed to images of confined spaces. This indicates that the response is neurologically conditioned rather than a matter of personal control.
💡Key Insight: Research shows that individuals with claustrophobia demonstrate stronger brain responses to boundary violations, or the sensation of personal space being intruded upon. This suggests that claustrophobia reflects a heightened sensitivity to perceived spatial threat rather than a mere weakness in coping.
💡Pro-Tip: If your fear seems connected to a specific memory or incident, gently working through that experience with support can help reduce its intensity over time. Avoidance may bring short-term relief, but addressing the root often leads to more lasting change.
Claustrophobia Treatment: How to Overcome Fear of Enclosed Spaces
Here is the most important thing we can tell you about claustrophobia: it is one of the most treatable mental health conditions that exists. Specific phobias, including claustrophobia, have among the highest treatment success rates of any anxiety disorder. Many people achieve significant, lasting recovery in a matter of weeks, sometimes even in a single extended session.
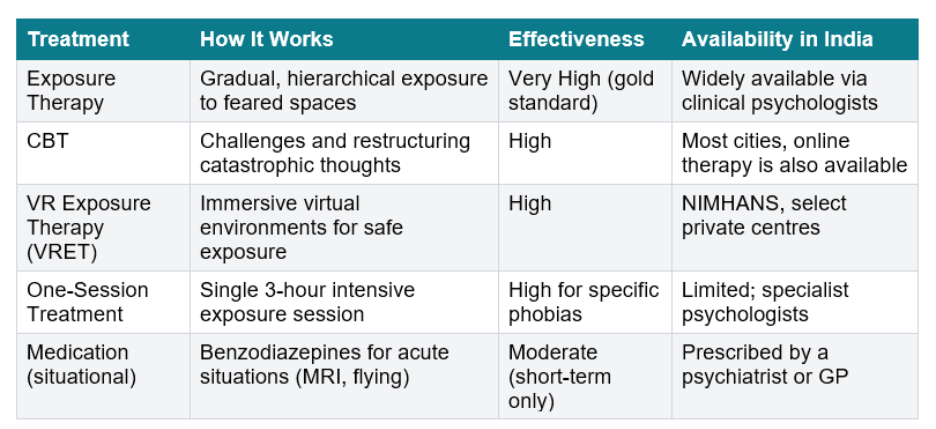
1. Exposure Therapy: The Gold Standard
Exposure therapy works by gradually and systematically introducing a person to feared situations, starting from the least distressing and progressing step by step.
For claustrophobia, a typical hierarchy might look like this:
- Imagining being in a small, enclosed room with the door closed
- Looking at photographs or videos of enclosed spaces
- Sitting in a small room with the door closed for gradually increasing periods
- Riding a lift alone for one floor
- Riding a lift alone for multiple floors
- Sitting in an MRI-like environment (some centres offer mock scanners)
- Completing the actual MRI scan
At each stage, the goal is to stay in the situation long enough for anxiety to rise and then naturally fall. This helps the brain learn that the situation is not actually dangerous, leading to a recalibration of the fear response over time.
2. Cognitive Behavioural Therapy (CBT)
CBT focuses on identifying and restructuring the thoughts that fuel anxiety.
People with claustrophobia often have automatic thoughts such as:
- “I won’t be able to breathe”
- “I’ll get trapped and won’t escape”
- “Something bad will happen if I stay here”
In therapy, these thoughts are:
- Examined for evidence
- Challenged for accuracy
- Replaced with more balanced alternatives
For example: “The space is enclosed, but it is ventilated and safe. This feeling is uncomfortable, not dangerous.”
CBT is often combined with exposure therapy, making it one of the most effective overall approaches.
3. Virtual Reality Exposure Therapy (VRET)
VRET uses immersive virtual environments to simulate enclosed spaces in a controlled, gradual manner.
Instead of immediately entering a real-life trigger, the person:
- Wears a VR headset
- Experiences simulated environments like elevators, tunnels, or MRI machines
- Progresses through increasing levels of confinement
This method is especially helpful for:
- People who feel too anxious to begin real-world exposure
- Situations that are difficult to recreate (e.g., MRI settings)
The brain often responds to virtual environments similarly to real ones, allowing desensitisation to occur safely.
4. One-Session Treatment (OST)
One-Session Treatment is an intensive form of exposure therapy completed in a single extended session (typically around 3 hours).
During this session:
- A trained psychologist guides the individual through the entire exposure hierarchy
- Cognitive restructuring is integrated throughout
- The person progresses rapidly from mild to more challenging situations
The goal is to:
- Break the avoidance cycle quickly
- Demonstrate that anxiety reduces without escape
- Build confidence in handling feared situations
OST has shown strong outcomes for specific phobias, especially when the fear is clearly defined, such as claustrophobia.
5. Medication (Situational Use)
Medication is typically not a long-term solution for claustrophobia but can be helpful in specific situations.
Commonly used options include:
- Short-acting anti-anxiety medications (e.g., benzodiazepines)
- Taken before high-stress situations like MRI scans or flights
These medications:
- Reduce immediate physical symptoms of anxiety
- Help the person tolerate the situation
However:
- They do not address the underlying fear
- They are usually used alongside therapy rather than as a standalone treatment
6. Self-Help Strategies for Mild Claustrophobia
For mild to moderate cases, structured self-help techniques can be effective:
- Diaphragmatic breathing: Breathe slowly into your belly (not your chest) for a count of four, hold for one count, exhale for six. Repeat five to ten times.
- 4-7-8 breathing technique: Inhale for 4 counts, hold for 7, exhale for 8. This activates the vagus nerve and quickly reduces heart rate.
- Grounding: Name five things you can see, four you can touch, three you can hear, two you can smell, and one you can taste. This anchors attention in the present rather than catastrophic thought.
- Cognitive reframing: When you notice the thought "the walls are closing in" or "I cannot breathe", counter it with: "The space is the same size it was a moment ago. I am safe. This feeling will pass."
- Progressive muscle relaxation: Tense and release muscle groups from feet to face. This reduces overall physical tension that fuels panic.
💡Pro Tip: If you are considering treatment, ask your therapist whether they use exposure-based approaches. Therapies that directly engage with the fear (rather than only talking about it) tend to produce faster and more lasting results in specific phobias like claustrophobia.
A Final Word
Priya, our software engineer from the opening of this article, did eventually get help. After three sessions of exposure therapy with a counselling psychologist, she was able to ride the metro to work. Not comfortably at first, but she got on.
Claustrophobia is not a character flaw or a sign of weakness. It is a well-understood and highly treatable anxiety response. If it is affecting your daily life, your health decisions, or your ability to get around, support can make a meaningful difference.
Through structured counselling and guided interventions, it is possible to gradually reduce fear and regain a sense of control.
Take the Next Step
If you or someone you know is struggling with claustrophobia, 1to1help’s Employee Assistance Program (EAP) offers:
- Confidential one-on-one counselling with trained psychologists
- Evidence-based approaches like CBT and exposure therapy
- Support for managing anxiety in real-life situations (e.g. travel, medical procedures)
- Referral pathways to psychiatrists or specialised care if required
Seeking support early can make the recovery process smoother and more manageable.
FAQs
Q1. What does claustrophobic mean?
"Claustrophobic" describes someone who experiences claustrophobia, which is an intense, irrational fear of enclosed or confined spaces. It is a specific phobia classified under anxiety disorders in the DSM-5. A claustrophobic person experiences severe anxiety, panic symptoms, and a desperate urge to escape when in small enclosed spaces like lifts, MRI machines, tunnels, or crowded rooms. In Hindi, this translates to "bund jagah se dar lagna" (fear of closed spaces). Claustrophobia is one of the most common specific phobias worldwide, affecting approximately 12.5% of the global population.
Q2. What is claustrophobic meaning in Hindi?
The claustrophobic meaning in Hindi relates to "संकुचित स्थानों का भय" (sankuchit sthaanon ka bhay) — the fear of enclosed or confined spaces. In everyday Hindi, it is often described as "bund jagah se dar lagna" (fear of closed places) or "tang jagah mein ghutan mehsoos hona" (feeling suffocated in a tight space). Claustrophobia is a treatable anxiety condition, and with the right therapy, particularly exposure therapy, most people can overcome it fully.
Q3. What triggers claustrophobia?
Claustrophobia is triggered by enclosed or confined spaces. The most common triggers include lifts (especially small, older ones), MRI scanners, crowded local trains, narrow corridors, underground tunnels, airplanes, small cars, and rooms without windows. In India, crowded public transport during peak hours are particularly common triggers. Anticipatory anxiety, the dread of a potentially claustrophobic situation, often begins hours before actual exposure. The severity depends on factors such as how confined the space is, how long the exposure lasts, and whether an accessible exit is visible.
Q4. Can a claustrophobic person have an MRI scan?
Yes. Claustrophobic patients can have MRI scans with the right preparation. Options in India include: (1) Open MRI machines that have no tunnel, available at select hospitals; (2) Wide-bore MRI (70cm) that is less confining than the standard 60cm machine; (3) A mild sedative or anxiolytic prescribed by the radiologist or referring doctor before the scan; (4) Breathing techniques and a staff member communicating with you throughout the procedure. Always inform your radiologist about your claustrophobia before booking. With proper preparation, the vast majority of claustrophobic patients can complete their MRI successfully.
Q5. Is claustrophobia curable?
Yes. Claustrophobia is highly treatable, and specific phobias have some of the best treatment outcomes of any mental health condition. The most effective approach is Exposure Therapy, which involves gradual, controlled exposure to feared enclosed spaces until the anxiety response diminishes. Many people achieve dramatic, lasting improvement even from a single extended exposure session (One-Session Treatment). CBT helps address the catastrophic thoughts that maintain the fear. Virtual Reality Exposure Therapy is increasingly available in India for claustrophobia. With proper treatment, most people can use lifts, complete MRI scans, and travel by public transport without debilitating fear.
Q6. What is the difference between claustrophobia and agoraphobia?
Claustrophobia and agoraphobia are opposite phobias. Claustrophobia is the fear of enclosed, confined spaces — lifts, tunnels, MRI machines, packed trains. Agoraphobia is the fear of open, public, or crowded spaces, often driven by a fear of not being able to escape or get help if something goes wrong. Both conditions cause significant avoidance and impact quality of life, and both are effectively treated with CBT and exposure therapy. It is possible, though relatively uncommon, for a person to have overlapping features of both conditions.
Q7. How can I manage claustrophobia on my own?
For mild claustrophobia, self-help can be effective. Begin with controlled breathing (diaphragmatic breathing or the 4-7-8 technique) to calm your nervous system when anxiety rises. Use grounding techniques: focus on what you can see, hear, and physically touch to stay anchored in the present. Gradually and voluntarily expose yourself to mildly claustrophobic situations, starting with imagined scenarios and working up to real-world ones. Challenge catastrophic thoughts: remind yourself that the lift is not getting smaller, and you have safely used enclosed spaces before. For moderate-to-severe claustrophobia, professional exposure therapy is significantly more effective and faster than self-help alone.
Recommended Readings
- BBC Three. (n.d.). What it’s like to live with claustrophobia. BBC. A first-person account that offers insight into the lived experience of claustrophobia and how it affects everyday situations. https://www.bbc.com/bbcthree/article/e7392d15-7edc-4cda-886e-0467177ea6c7
- The Recovery Village. (n.d.). 5 common myths about claustrophobia debunked. Explains common misconceptions about claustrophobia, including the difference between discomfort and clinical phobia, and highlights that it is a treatable condition. https://www.therecoveryvillage.com/mental-health/claustrophobia/claustrophobia-myths/
- News-Medical. (n.d.). Claustrophobia research. Summarises current research on claustrophobia, including brain mechanisms, spatial perception, and the triggers and maintenance of fear responses. https://www.news-medical.net/health/Claustrophobia-Research.aspx
- Max Healthcare. (n.d.). Crowd (un)pleaser: Claustrophobia in crowds. Explores how claustrophobia can extend beyond enclosed spaces to crowded environments, highlighting the role of perceived lack of control and restricted movement in triggering anxiety. https://www.maxhealthcare.in/blogs/crowd-unpleaser-claustrophobia-crowds
References
- American Psychiatric Association. (n.d.). Diagnostic and statistical manual of mental disorders (DSM-5).
https://www.psychiatry.org/psychiatrists/practice/dsm
- Calmerry. (n.d.). What is claustrophobia: Everything you need to know.
https://calmerry.com/blog/anxiety/what-is-claustrophobia-everything-you-need-to-know/
- Cleveland Clinic. (n.d.). Amygdala.
https://my.clevelandclinic.org/health/body/24894-amygdala
- Cleveland Clinic. (n.d.). Anxiety disorders.
https://my.clevelandclinic.org/health/diseases/9536-anxiety-disorders
- Cleveland Clinic. (n.d.). Benzodiazepines (benzos).
https://my.clevelandclinic.org/health/treatments/24570-benzodiazepines-benzos
- Cleveland Clinic. (n.d.). Claustrophobia.
https://my.clevelandclinic.org/health/diseases/21746-claustrophobia
- Cleveland Clinic. (n.d.). Diaphragmatic breathing.
https://my.clevelandclinic.org/health/articles/9445-diaphragmatic-breathing
- Cleveland Clinic. (n.d.). Vagus nerve.
https://my.clevelandclinic.org/health/body/22279-vagus-nerve
- Fortis Healthcare. (n.d.). What is claustrophobia: Causes, symptoms, and treatment options.
https://www.fortishealthcare.com/blogs/what-claustrophobia-causes-symptoms-and-treatment-options
- HealthTree Foundation. (n.d.). 4-7-8 breathing to reduce anxiety.
https://healthtree.org/myeloma/community/articles/myeloma-patients-4-7-8-breathing-reduce-anxiety
- Mayo Clinic. (n.d.). MRI.
https://www.mayoclinic.org/tests-procedures/mri/about/pac-20384768
- Mayo Clinic. (n.d.). Agoraphobia.
https://www.mayoclinic.org/diseases-conditions/agoraphobia/symptoms-causes/syc-20355987
- Mayo Clinic. (n.d.). Panic attacks.
https://www.mayoclinic.org/diseases-conditions/panic-attacks/symptoms-causes/syc-20376021
- Mayo Clinic. (n.d.). Post-traumatic stress disorder (PTSD).
https://www.mayoclinic.org/diseases-conditions/post-traumatic-stress-disorder/symptoms-causes/syc-20355967
- Max Healthcare. (n.d.). Crowd (un)pleaser: Claustrophobia in crowds.
https://www.maxhealthcare.in/blogs/crowd-unpleaser-claustrophobia-crowds
- MSKCC (Memorial Sloan Kettering Cancer Center). (n.d.). CT vs MRI: What’s the difference?
https://www.mskcc.org/news/ct-vs-mri-what-s-difference-and-how-do-doctors-choose-which-imaging-method-use
- MXR Imaging. (n.d.). Wide bore MRI systems.
https://mxrimaging.com/blogs/wide-bore-mri-systems/
- National Center for Biotechnology Information. (n.d.). MRI contraindications.
https://www.ncbi.nlm.nih.gov/books/NBK551669/
- National Institutes of Health. (n.d.). Reduction of claustrophobia during MRI.
https://pmc.ncbi.nlm.nih.gov/articles/PMC3045881/
- National Institutes of Health. (n.d.). Sedation for MRI procedures.
https://pmc.ncbi.nlm.nih.gov/articles/PMC10118336/
- RadiologyInfo.org. (n.d.). MRI safety.
https://www.radiologyinfo.org/en/info/safety-mr
- ResearchGate. (n.d.). Near space and its relation to claustrophobic fear.
https://www.researchgate.net/publication/50374836_Near_space_and_its_relation_to_claustrophobic_fear
- ScienceDirect. (n.d.). Supporting claustrophobic patients during MRI.
https://www.sciencedirect.com/science/article/pii/S1078817423002067
- United We Care. (n.d.). How to overcome claustrophobia.
https://www.unitedwecare.com/how-to-overcome-claustrophobia/
- U.S. Department of Veterans Affairs. (n.d.). Progressive muscle relaxation.
https://www.va.gov/WHOLEHEALTHLIBRARY/tools/progressive-muscle-relaxation.asp
- Verywell Mind. (n.d.). Claustrophobia.
https://www.verywellmind.com/claustrophobia-2671681
- Verywell Mind. (n.d.). Diagnosing a specific phobia.
https://www.verywellmind.com/diagnosing-a-specific-phobia-2671981
- Verywell Mind. (n.d.). Fight-or-flight response.
https://www.verywellmind.com/what-is-the-fight-or-flight-response-2795194
- Verywell Mind. (n.d.). Cognitive reframing.
https://www.verywellmind.com/reframing-defined-2610419
- Virtual CBT. (n.d.). Exposure therapy for claustrophobia.
https://www.virtualcbt.ca/therapy-blog/exposure-therapy-claustrophobia
- Wikipedia contributors. (n.d.). Safety of magnetic resonance imaging.
https://en.wikipedia.org/wiki/Safety_of_magnetic_resonance_imaging