
.png)

Mental Health Concerns
Eating Disorders: Types, Symptoms, Causes & Treatment - India Guide 2026

.png)
Written by
Aarohi Parakh,
Psychologist and Content Writer

Reviewed by
Sanjana Sivaram,
Psychologist and Clinical Content Head






Introduction
Ananya is a 19-year-old engineering student in Chennai. Her college hostel has a canteen, but she rarely goes there. She has been eating alone in her room for the past four months, measuring every gram of rice and cross-referencing every ingredient with an app on her phone. She has lost eight kilograms since joining college. Her family, on a recent video call, told her she was looking "fit and healthy". She smiled and said nothing.
Ananya is not dieting. She is not disciplined. She is living with anorexia nervosa, and nobody around her has recognised it. That gap between what is happening and what is seen is the central challenge of eating disorders in India.
Eating disorders are serious, potentially life-threatening mental health conditions. They are not lifestyle choices. They are not just phases. And they are not, as is widely assumed in India, a Western concept that does not affect people here. This guide covers the definition, types of eating disorders, symptoms, causes, and treatment options, with a specific focus on how eating disorders present and are understood in the Indian context.

What Are Eating Disorders? Definition and Overview
Eating disorders definition: Eating disorders are serious mental health conditions characterised by persistent disturbances in eating behaviour, accompanied by distressing and intrusive thoughts and emotions about food, body weight, and body image. They affect how a person eats, how they relate to their body, and how much psychological space food and weight occupies in daily life.
Critically, eating disorders are not choices, not phases, not vanity, and not the result of weak willpower. They are complex psychiatric illnesses with biological, psychological, and social roots. The DSM-5 TR (American Psychiatric Association) classifies them under Feeding and Eating Disorders, a category that includes conditions ranging from anorexia nervosa, bulimia nervosa, binge eating disorder, to the less commonly known Avoidant/Restrictive Food Intake Disorder (ARFID) and Pica.
Eating disorders, as per DSM, are characterised by the “persistent disturbance of eating or eating-related behaviour that results in the altered consumption or absorption of food and that significantly impairs physical health or psychosocial functioning”.
The overall lifetime prevalence of eating disorders is estimated to be 8.60% among females and 4.07% among males. In India, the picture is complicated by underdiagnosis: the conditions are frequently misread as religious fasting, disciplined dieting, or "healthy eating", cultural framings that provide cover for what could be increasingly dangerous patterns.
India Focus: Eating disorders in India are not uncommon. They are underreported. Rapid urbanisation, social media penetration, changing beauty standards influenced by Bollywood and international media, and intense academic and professional competition have created conditions in which eating disorders are growing, particularly among urban youth aged 13-30. The absence of India-specific large epidemiological data does not mean absence of the condition.
Types of Eating Disorders: A Complete Guide
Understanding the types of eating disorders is essential for accurate identification and appropriate treatment. Each type has a distinct profile of symptoms, risks, and treatment approaches. What they share is the presence of disordered eating behaviour combined with significant psychological distress around food, eating, and body image.

Anorexia Nervosa
Anorexia nervosa is characterised by extreme restriction of food intake, an intense and persistent fear of gaining weight, and a severely distorted perception of one's body size. People with anorexia typically see themselves as overweight even when dangerously underweight. Anorexia is the deadliest eating disorder, with a mortality rate of 5-10% from medical complications including cardiac arrest, electrolyte imbalances, and multi-organ failure.
It presents in two subtypes: the restrictive type (food restriction only) and the binge-purge type (restriction combined with occasional bingeing and purging).
Purging refers to behaviors used to “get rid of” calories after eating. In simple terms, it includes actions like self-induced vomiting, misuse of laxatives or diuretics, or excessive exercise to prevent weight gain. In India, anorexia is most commonly seen in young women, though it affects men and all genders. The condition is frequently missed because significant weight loss is celebrated rather than questioned.
Case Example: Riya, a 19-year-old college student in Mumbai, began “eating clean” to lose a few kilograms before a college event. Over months, her intake reduced drastically to salads and black coffee. Despite visible weight loss, her family praised her discipline. Riya avoided family meals, exercised excessively, and repeatedly checked her body in mirrors. Even when her BMI dropped into a medically concerning range and she experienced missed periods and dizziness, she insisted she was “still fat.” She was brought for consultation only after fainting episodes.
Bulimia Nervosa
Bulimia nervosa involves cycles of binge eating (consuming large amounts of food rapidly, with a feeling of loss of control) followed by compensatory behaviours or purging intended to prevent weight gain. These compensatory behaviours include self-induced vomiting, misuse of laxatives, excessive exercise, or fasting. Unlike anorexia, people with bulimia are often at a normal or higher-than-average body weight, making the condition significantly harder to detect visually.
In India, dental erosion (from stomach acid), swollen jaw or cheeks (parotid gland enlargement), and the characteristic knuckle calluses known as Russell's sign are physical markers that GPs should be trained to identify, as patients with bulimia are unlikely to disclose the behaviour voluntarily.
Case Example: Aman, a 24-year-old working in a corporate role in Gurgaon, reported frequent throat irritation and dental sensitivity. On further assessment, he described episodes of eating large quantities of food late at night after stressful workdays, followed by self-induced vomiting. He maintained a normal body weight and high work performance, which delayed suspicion. Physical signs like enamel erosion and calluses on his knuckles eventually prompted a referral.
Binge Eating Disorder (BED)
Binge eating disorder involves recurrent episodes of eating large amounts of food with a feeling of loss of control, followed by significant distress, guilt, and shame, but without the compensatory purging behaviours seen in bulimia. BED is strongly associated with obesity, depression, and anxiety, and is rising in India alongside the growing urban obesity epidemic.
BED is particularly under-identified in India because episodes of overeating are normalised in cultural contexts around festivals, family meals, and stress. The clinical distinction is in the loss of control and the sustained psychological distress that follows.
Case Example: Neha, a 32-year-old homemaker in Ahmedabad, described repeated episodes of eating large amounts of food in secrecy, especially during afternoons when alone. These episodes were accompanied by a sense of loss of control and followed by intense guilt and self-criticism. Her family attributed her weight gain to “lack of willpower,” while she struggled with low mood and withdrawal. Unlike bulimia, she did not engage in purging behaviours.
ARFID (Avoidant/Restrictive Food Intake Disorder)
ARFID is characterised by extreme food selectivity based on sensory features such as texture, colour, smell, or appearance, rather than body image or weight concerns. Children and adolescents with ARFID may eat only a very narrow range of foods and can develop nutritional deficiencies serious enough to require medical intervention. ARFID is more common in children on the autism spectrum or with sensory processing differences and is increasingly recognised in Indian child psychiatry settings.
Case Example: Kabir, a 7-year-old child in Bengaluru, ate only a very limited range of foods, primarily plain rice, biscuits, and milk. He refused foods based on texture and smell, often gagging when pressured to try new items. His growth began to plateau, and nutritional deficiencies were identified. Kabir also had sensory sensitivities and was later evaluated for neurodevelopmental differences, leading to a diagnosis consistent with ARFID.
Orthorexia
Orthorexia is not yet formally classified in the DSM-5, but it is increasingly prevalent in India's urban, health-conscious communities. It involves an obsessive fixation on eating 'correctly', 'purely', or 'cleanly', to the point where rigid food rules dominate daily life, cause significant anxiety, and result in nutritional deficiency. In India, orthorexia frequently presents through the language of Ayurveda, yoga, or 'sattvic' diets, making it particularly difficult to distinguish from genuine wellness practice without clinical assessment. The International Journal of Indian Psychology has noted its rising prevalence among young urban professionals. It should be noted that while not a formal diagnosis yet as per DSM, it can still cause significant distress and impact on daily functioning.
Case Example: Sneha, a 28-year-old yoga instructor in Pune, became increasingly rigid about consuming only “pure” and “sattvic” foods. She eliminated multiple food groups, avoided eating outside, and experienced anxiety if her dietary rules were disrupted. What began as a wellness practice escalated into social withdrawal and nutritional imbalance. She did not express fear of weight gain, but her identity and daily functioning became dominated by food rules.
Pica
Pica involves the persistent consumption of non-food items including soil (geophagy), chalk, ice, paper, or clay. In India, Pica is more prevalent than commonly acknowledged, particularly in pregnant women and young children in rural and semi-urban settings, where it is often linked to iron, zinc, or calcium deficiency. Cultural practices around consuming clay or mud during pregnancy in some Indian regions overlap with Pica in ways that require culturally sensitive clinical assessment.
Case Example: Sunita, a 26-year-old pregnant woman in a semi-urban area near Varanasi, reported persistent cravings to eat मिट्टी (mud) during her second trimester. Initially dismissed as a common pregnancy craving, the behaviour became frequent and compulsive. Medical evaluation revealed iron deficiency anemia. With nutritional intervention and psychoeducation, the behaviour reduced.
Night Eating Syndrome (NES)
Night Eating Syndrome is characterised by delayed circadian eating patterns, including consuming a significant portion of daily calories after dinner, frequent night awakenings to eat, and morning appetite suppression. Occasional night eating is common. But night eating syndrome doesn’t just happen every once in a while. It happens several times per week, often with multiple wakeups per night. Night eating syndrome is an eating disorder that happens alongside a sleep disorder (insomnia).
Case Example: Rohit, a 30-year-old IT professional in Hyderabad, reported minimal appetite during the day but consumed large meals late at night, often waking up to eat again. His sleep was fragmented, and he experienced fatigue and irritability during work hours. He did not report binge episodes with loss of control, but rather a consistent pattern of night eating linked to stress and irregular work schedules.
OSFED (Other Specified Feeding or Eating Disorder)
OSFED includes clinically significant eating disorder presentations that do not meet full criteria for anorexia, bulimia, or BED but still cause distress and impairment. In some cases, this is because the frequency of the behavior does not meet the diagnostic threshold (e.g., the frequency of binges in bulimia or binge eating disorder) or the weight criteria for the diagnosis of anorexia nervosa are not met.
Case Example: Megha, a 22-year-old student in Delhi, maintained a normal weight but engaged in frequent restrictive eating during weekdays and occasional purging behaviours after perceived overeating. Her symptoms did not meet the full diagnostic threshold for anorexia or bulimia, but she experienced intense body dissatisfaction, anxiety around food, and significant disruption to her daily functioning. She was diagnosed with OSFED.
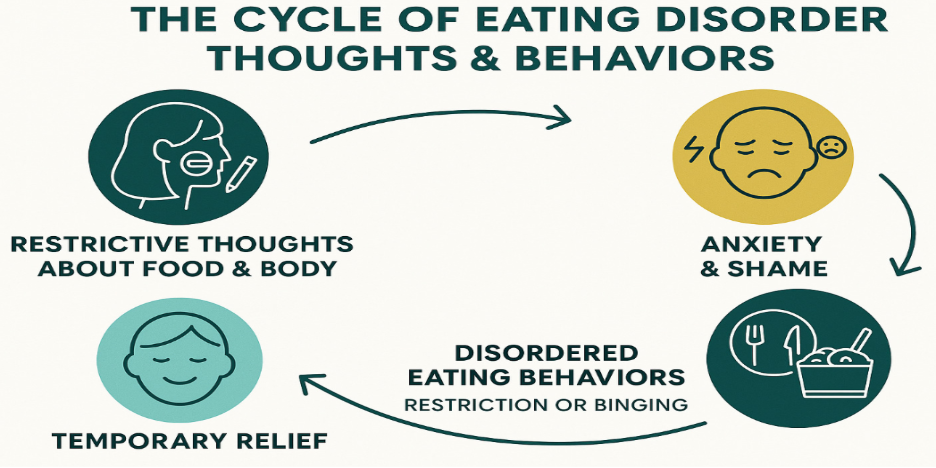
Eating Disorder Symptoms: Warning Signs to Watch For

Symptoms of eating disorders span the physical, behavioural, psychological, and cultural dimensions of a person's daily life. One of the reasons eating disorders go undetected in India for so long is that many of the warning signs are either culturally reframed as virtues (discipline, restraint, health-consciousness) or are attributed to physical illness rather than a mental health condition
Eating Disorders in Adolescents and Children
Eating disorders in adolescence are a particular concern given the combination of social media exposure, body image pressure, and competitive academic environments. Research shows rising referrals for eating disorders among adolescents aged 10-19 in urban centres. Early identification in schools and by parents is critical.
Eating disorders in children most commonly present as ARFID or Pica, though restrictive patterns that precede anorexia can begin in childhood. School counsellors and paediatricians in India are often the first point of contact, and training in recognising eating disorder warning signs in these settings remains inadequate.
Eating Disorders Test: Validated Screening Tools
The SCOFF questionnaire is a widely used 5-question screening tool for eating disorders, validated for use in India. If you answer 'yes' to 2 or more questions, further professional assessment is strongly recommended. The EDE-Q (Eating Disorder Examination Questionnaire) is the gold-standard self-report measure for symptom severity. Both tools are available free of charge via the National Alliance for Eating Disorders at allianceforeatingdisorders.com. These tools are starting points, not diagnoses. A clinical assessment from a trained psychologist or psychiatrist is needed for diagnosis.
When to Seek Professional Help
Awareness is important, but recognising when to act is critical.
You should consider seeking professional help if:
- Eating patterns are becoming rigid, restrictive, or out of control
- There is noticeable weight change or physical health impact
- Thoughts about food, body, or weight feel overwhelming or constant
- Eating behaviours are affecting social life, work, or academics
- There are behaviours such as purging, bingeing, or excessive exercise
- You feel unable to change these patterns despite wanting to
For Parents and Caregivers: early signs such as meal avoidance, anxiety around food, or sudden dietary rigidity should not be dismissed as a phase. Act early. Speak to a qualified professional or consider reaching out to a trusted mental health helpline for initial support. Early intervention leads to better recovery outcomes.
What Causes Eating Disorders in India?
Causes of eating disorders are never singular. They develop through the intersection of biological vulnerability, psychological patterns, family dynamics, and cultural and social pressures. In India, several of these pressures are distinct and intensified in ways that existing Western research does not fully capture.
Biological Factors
- Genetics:
- Anorexia nervosa shows ~50–80% heritability
- Family history of eating disorders, OCD, or high perfectionism increases risk
- Brain Chemistry:
- Impacts appetite regulation, mood, impulse control, and reward processing
Psychological Factors
- Perfectionism:
- High-pressure academic environments such as JEE, NEET, and UPSC preparation
- Perfectionistic tendencies may extend from academics to body image and eating
- Low Self-Esteem:
- Reinforced by family comments about weight or appearance
- Early experiences of teasing, bullying, or academic comparison
- Trauma and Adverse Childhood Experiences (ACEs):
- Physical, emotional, or sexual abuse
- Bullying, especially related to body or appearance
Social and Cultural Factors (India-Specific Context)
- Social Media Exposure:
- High engagement with platforms like Instagram and YouTube
- Exposure to “clean eating,” weight loss transformations, and unrealistic body standards
- Algorithm-driven content can reinforce comparison and body dissatisfaction
- Appearance-Based Social Pressures:
- Cultural emphasis on thinness and fairness, especially for women
- External validation linked to appearance in social and familial contexts
- Fear of Social Judgment (“Log kya kahenge”):
- Pressure to conform to socially acceptable body standards
- Can lead to both restrictive eating and secrecy around disordered behaviours
- Religious and Cultural Fasting Practices:
- Fasting may sometimes mask or reinforce restrictive eating patterns
- Particularly relevant in individuals already vulnerable to control-based eating behaviours
Family and Environmental Factors
- Family Dynamics:
- Critical comments about weight, food, or appearance
- High expectations around achievement and discipline
- Comorbid Mental Health Conditions:
- OCD, anxiety disorders, depression, and PTSD commonly co-occur
- These conditions can both contribute to and be worsened by eating disorders
Vulnerable Groups and Minority Stress
- Emerging research indicates higher risk of eating disorders among LGBTQ+ individuals
- Contributing factors include body image pressures, identity-related stress, stigma, and social rejection
- In the Indian context, limited access to affirming mental health support may further increase vulnerability

💡Pro-tip for Parents:
- Notice early signs such as:
- Sudden interest in “clean eating” or rigid food rules
- Calorie counting or eliminating entire food groups
- Increased anxiety around meals
- Avoid immediately praising these behaviours as discipline
- Start open conversations instead of confrontation
- Involve a school counsellor or mental health professional if patterns persist or escalate
Eating Disorders in India: The Cultural Blind Spot
In many Indian families, eating disorders are still associated with extreme or visibly severe cases, often shaped by Western media portrayals. As a result, early or less obvious signs may be overlooked. These can include rigid “healthy eating,” excessive exercise, or unusual cravings during pregnancy that are dismissed as normal or even praised.
This gap between common perceptions and how eating disorders actually present in everyday life can delay identification and access to care.
Why Eating Disorders Go Undetected in India
- Cultural framing: eating disorders are widely seen as a 'Western problem' with no relevance to Indian families
- Normalisation of restriction: food restriction is frequently mistaken for discipline, good character, or religious devotion
- Fasting practices: Periodic fasting is a common cultural and spiritual practice in India. In some cases, it may unintentionally reinforce or mask restrictive eating patterns in individuals who are already vulnerable.
- Family enabling: weight loss is often praised ('you are looking so fit!') rather than questioned, particularly if the person was previously considered overweight
- Clinical training gaps: many Indian GPs and paediatricians have not received adequate training in identifying eating disorder symptoms, particularly the subtler presentations of bulimia, BED, and ARFID. This may lead to a delay in referral to clinical psychologists or psychiatrists.
- Stigma: seeking help for food-related psychological distress carries the dual stigma of mental health and of appearing obsessed with appearance
Daycare and Treatment for Children with Eating Disorders in India
For parents searching for daycare or structured treatment options for children with eating disorders in India, it is important to know that formal, specialised day treatment programmes for paediatric eating disorders remain limited.
- Leading public institutions such as National Institute of Mental Health and Neurosciences (NIMHANS) and All India Institute of Medical Sciences (AIIMS) offer child and adolescent psychiatry services that can manage eating disorders through structured outpatient care, and in some cases, day programme formats.
- In metro cities, private child psychiatrists and multidisciplinary teams (including psychologists, nutritionists, and paediatricians) can design individualised outpatient treatment plans that function similarly to day treatment. These often include:
- Regular therapy sessions
- Nutritional rehabilitation and monitoring
- Family-based interventions
- School coordination where required
- For families who may not have access to specialised centres, starting with a paediatrician or mental health professional can help initiate appropriate referrals and care pathways.
Support for Parents, Families, and Individuals (Including EAP Counselling)
Eating disorders affect not just the individual but the entire family system. Parents and caregivers often experience confusion, guilt, and high levels of stress while trying to support recovery.
- Employee Assistance Programs (EAPs) offered by many organisations in India, such as 1to1help, can provide:
- Confidential counselling for parents or family members
- Guidance on how to support a loved one with an eating disorder
- Referrals to specialised mental health services
- Emotional support for caregivers navigating ongoing care
- EAP services can also be accessed by individuals experiencing early or mild symptoms, especially when concerns around food, body image, or control are beginning to cause distress.
- If additional support is needed, you can contact the Government of India’s Tele-MANAS helpline (14416) for free, confidential mental health assistance.
Eating Disorders in Men in India
Eating disorders in Indian men are significantly underdiagnosed. The misconception that they primarily affect women prevents both help-seeking and timely diagnosis.
In men, disordered eating may present as:
- Muscle dysmorphia (extreme focus on muscularity through rigid diet and excessive exercise)
- Binge eating disorder
- Night eating syndrome
These behaviours are often misinterpreted as discipline or fitness commitment, which can delay recognition.
If you notice concerning patterns in your relationship with food, exercise, or body image, reaching out for support, including through EAP services or helplines, can be an important first step.
💡Key Takeaway: Early intervention and a multidisciplinary approach are critical. Even when formal daycare programmes are limited, structured outpatient care combined with family involvement can be highly effective.
For managers and workplaces: If someone on your team appears to be losing significant weight, consistently skipping meals, or expressing a strong preoccupation with food or body image, approach them with empathy and curiosity rather than commenting on their appearance. Supportive conversations can make it easier for individuals to seek help.
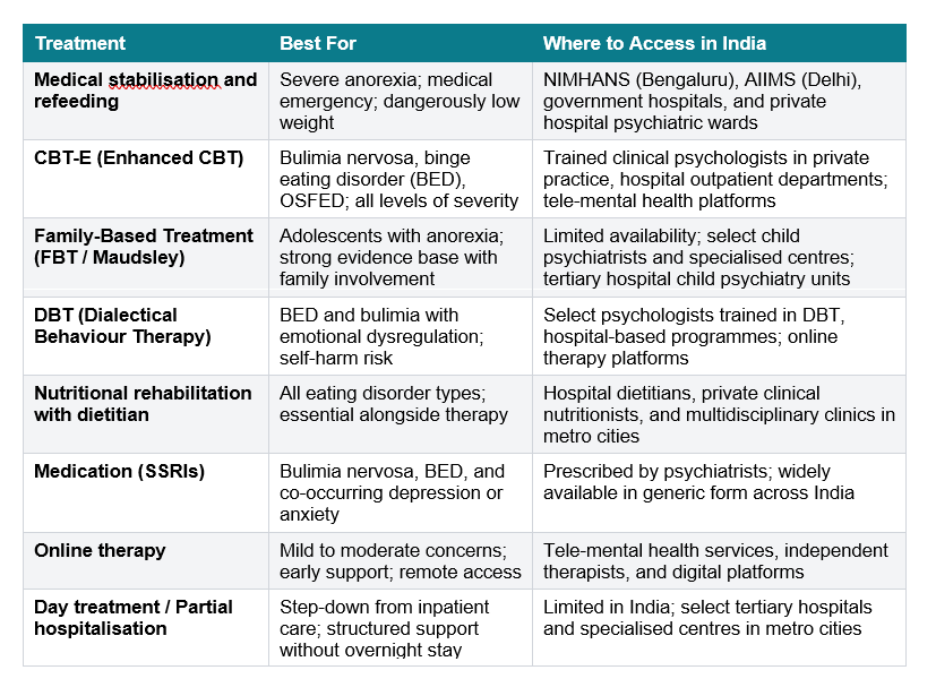
Eating Disorder Treatment in India: Options and Resources
Treatment for eating disorders is most effective when it is multidisciplinary: a psychiatrist, a clinical psychologist, and a specialist dietitian working together. This team approach addresses the medical, psychological, and nutritional dimensions of the condition simultaneously, as all three interact.
Emergency and Immediate Support
- If there is medical instability (fainting, severe weakness, electrolyte imbalance, rapid weight loss), seek urgent care at the nearest hospital emergency department
- For immediate mental health support, you can contact the Government of India’s Tele-MANAS helpline (14416), which provides free, 24/7 mental health assistance
CBT-E: The Most Evidence-Based Psychological Treatment
Enhanced Cognitive Behavioural Therapy (CBT-E), developed by Professor Christopher Fairburn at the University of Oxford, is the most evidence-based psychological treatment for eating disorders and is suitable for anorexia, bulimia, BED, and OSFED. It directly addresses the cognitive processes that maintain disordered eating: overvaluation of shape and weight, perfectionism, low self-esteem, and interpersonal difficulties. CBT-E is available from trained clinical psychologists in India and increasingly through online therapy platforms for mild to moderate presentations.
Family-Based Treatment: Particularly Relevant in India
Family-Based Treatment (FBT), also called the Maudsley Approach, is particularly effective for adolescents with anorexia and maps well onto India's family-centric culture. In the first phase, parents take an active role in re-feeding their child, removing the responsibility for eating decisions from the person with the eating disorder. In later phases, autonomy is gradually restored. FBT requires a therapist trained in the approach; it is available from select child psychiatrists in major Indian cities and through some private clinical psychologists.
Dialectical Behaviour Therapy (DBT)
- Best suited for individuals with binge eating or bulimia who also struggle with emotional dysregulation, impulsivity, or self-harm
- Focuses on distress tolerance, emotion regulation, and interpersonal effectiveness
- Increasingly available in India through trained psychologists and structured therapy programmes
Nutritional Rehabilitation and Counselling
- Core component across all eating disorders
- Involves structured meal planning, normalising eating patterns, and correcting nutritional deficiencies
- Delivered by clinical dietitians in coordination with therapists and psychiatrists
- Especially critical in anorexia and ARFID, where medical risk is high
Interpersonal Psychotherapy (IPT)
- Particularly effective for binge eating disorder (BED)
- Targets interpersonal stressors such as role transitions, conflicts, and social isolation that maintain disordered eating
- Useful when eating behaviours are closely linked to relationship difficulties
Pharmacotherapy (Medication)
- Typically used as an adjunct to therapy, not a standalone treatment
- Selective Serotonin Reuptake Inhibitors (SSRIs) may be prescribed for bulimia, BED, and co-occurring depression or anxiety
- Limited role in anorexia, except for managing comorbid conditions
- Requires ongoing monitoring by a psychiatrist
Inpatient Treatment / Hospitalisation
- Required in cases of medical instability, severe malnutrition, or high psychiatric risk
- Focuses on medical stabilisation, supervised refeeding, and close monitoring
- Available in tertiary hospitals and specialised psychiatric units in India
Group Therapy and Support Groups
- Provides peer support, shared experiences, and reduced isolation
- Often used alongside individual therapy
- Can be helpful in recovery and relapse prevention phases
School-Based and Family Interventions (for Children & Adolescents):
- Involves school counsellors, teachers, and caregivers
- Focuses on routine stabilisation, reducing academic pressure, and monitoring eating patterns
- Particularly relevant in the Indian context where academic environments are high-pressure
Prevention of Eating Disorders in India
Prevention of eating disorders requires interventions at multiple levels.
- At the school level: media literacy programmes that teach critical evaluation of body image content; teacher training to identify early warning signs; non-stigmatising health education that separates health behaviours from appearance.
- At the family level: eliminating comments about children's weight and appearance; modelling a balanced relationship with food; treating religious fasting as spiritually meaningful rather than an opportunity for restriction.
- At the societal level: regulation of extreme thinness in Bollywood and advertising; social media platforms proactively suppressing harmful body image content.

A Final Word
Ananya, the engineering student from our opening, eventually spoke to a counsellor at her college’s wellness centre. The counsellor used the SCOFF questionnaire. Ananya answered yes to four out of five questions. It was the first time she had a name for what she had been living with for nearly two years.
Naming it was not a cure. But it was the beginning of one.
Eating disorders in India are real, they are growing, and they are treatable. The silence around them, driven by stigma, cultural misreading, and gaps in awareness, often delays help-seeking and prolongs distress that could be addressed earlier.
If something in this guide feels familiar, reaching out is an important first step.
- Call the Government of India’s Tele-MANAS helpline (14416) for free, 24/7 support in multiple Indian languages
- Use brief screening tools like the SCOFF questionnaire to reflect on your symptoms
- Access Employee Assistance Programme (EAP) counselling, which offers confidential support for individuals and families dealing with concerns around food, body image, or mental health
- Organisations such as 1to1help provide EAP counselling services, along with structured support like 1to1parenting cohort-based programmes for parents managing stress related to their child’s eating behaviours or emotional well-being
FAQs
Q1. What are eating disorders?
Eating disorders are serious mental health conditions characterised by persistent disturbances in eating behaviour, accompanied by intense and distressing thoughts about food, body weight, and appearance. They include anorexia nervosa (extreme food restriction), bulimia nervosa (binge-purge cycles), and binge eating disorder (loss-of-control overeating). Eating disorders have one of the highest mortality rate of any psychiatric condition. In India, they are significantly underdiagnosed, partly because they are mistakenly seen as a “Western problem” or confused with disciplined dieting or fasting practices. They affect people of all genders, ages, and body sizes.
Q2. What are the types of eating disorders?
The main types of eating disorders are:
- Anorexia Nervosa: extreme restriction and intense fear of weight gain
- Bulimia Nervosa: binge-purge cycles, often at a normal weight
- Binge Eating Disorder (BED): loss-of-control eating without purging; most prevalent
- ARFID: extreme food selectivity based on sensory features, not body image
- Orthorexia: obsessive fixation on “healthy” or “clean” eating (not yet a formal diagnosis)
- Pica: consumption of non-food items
- OSFED: clinically significant symptoms that do not meet full criteria for other disorders
All types benefit from multidisciplinary professional treatment.
Q3. What causes eating disorders?
Eating disorders develop through a combination of biological, psychological, and social factors. Genetically, anorexia shows high heritability. Psychologically, factors such as perfectionism, low self-esteem, trauma, and anxiety increase vulnerability. In India, additional influences can include appearance-related pressures, social media exposure, family comments about weight, and cultural contexts that may unintentionally normalise restrictive eating. Causes are rarely singular, and effective treatment addresses multiple contributing factors.
Q4. What are the warning signs of an eating disorder?
Warning signs include:
- Significant weight loss or frequent fluctuations
- Avoiding family meals or disappearing after eating
- Obsessive calorie counting or rigid food rules
- Hair loss, dental issues, fainting, or fatigue
- Excessive exercise despite illness or injury
- Intense fear of certain foods or weight gain
- Guilt, shame, or distress after eating
In India, also watch for persistent avoidance of shared meals or rigid “clean eating” patterns that interfere with daily life. These signs warrant a professional assessment rather than casual reassurance.
Q5. How are eating disorders treated in India?
Treatment typically involves a multidisciplinary team:
- Psychiatrist (medical monitoring, medication if needed)
- Clinical psychologist (CBT-E, DBT, or other therapies)
- Dietitian (nutritional rehabilitation)
For adolescents, Family-Based Treatment (FBT) is particularly effective. Severe cases may require hospitalisation. While specialised centres are limited, treatment is available through tertiary hospitals such as NIMHANS and AIIMS, as well as private practitioners and online therapy services.
Q6. Are eating disorders common in India?
Yes. Eating disorders are increasingly recognised in India, particularly among adolescents and young adults, though they remain underdiagnosed. Contributing factors include changing body ideals, increased social media exposure, academic pressure, and evolving lifestyle patterns. Binge eating disorder is also rising alongside increasing rates of obesity. Limited national data reflects a research gap rather than low prevalence.
Q7. Can eating disorders affect men in India?
Yes. Eating disorders affect men as well, but are often underdiagnosed due to stigma and the misconception that they primarily affect women. In men, presentations may include muscle dysmorphia, binge eating disorder, and night eating syndrome, often masked as fitness or lifestyle behaviours.
If you recognise concerning patterns in your relationship with food, body image, or exercise:
- Contact the Government of India’s Tele-MANAS helpline (14416) for free, confidential support
- Consider accessing Employee Assistance Programme (EAP) counselling, which offers private support for individuals and families
- Organisations such as 1to1help provide confidential EAP counselling and guidance for mental health concerns
Additional Resources
1. National Alliance for Eating Disorders: Family Toolkit: Guide for parents and families supporting a loved one with an eating disorder- https://www.nationaleatingdisorders.org/wp-content/uploads/2012/06/ParentToolkit-946.pdf
2. The Eating Disorder Recovery Handbook by Nicola Davies and Emma Bacon: This book offers practical advice, exercises, and support for those recovering from eating disorders.
3. 8 Keys to Recovery from an Eating Disorder by Carolyn Costin and Gwen Schubert Grabb: A step-by-step guide that provides tools for recovery, including personal stories, exercises, and strategies.
References
- American Psychiatric Association. (n.d.). What are eating disorders? https://www.psychiatry.org/patients-families/eating-disorders/what-are-eating-disorders
- Avasthi, A., et al. (2021). Eating disorders in India: An overview. Indian Journal of Psychiatry. https://journals.lww.com/aips/fulltext/2021/05010/eating_disorders_in_india__an_overview.3.aspx
- Cleveland Clinic. (2024, December 4). Diuretics (water pills): Types, uses & side effects. Diuretics (water pills): Types, uses & side effects
- Cleveland Clinic. (n.d.). Laxatives: What they are, types & how they work. https://my.clevelandclinic.org/health/treatments/25121-laxatives
- Cleveland Clinic. (n.d.). Eating disorders. https://my.clevelandclinic.org/health/diseases/4152-eating-disorders
- Cleveland Clinic. (n.d.). Binge eating disorder. https://my.clevelandclinic.org/health/diseases/17652-binge-eating-disorder
- Cleveland Clinic. (n.d.). Avoidant/restrictive food intake disorder (ARFID). https://my.clevelandclinic.org/health/diseases/24869-arfid-avoidant-restrictive-food-intake-disorder
- Cleveland Clinic. (n.d.). Pica. https://my.clevelandclinic.org/health/diseases/22944-pica
- Cleveland Clinic. (n.d.). Night eating syndrome (NES). https://my.clevelandclinic.org/health/diseases/21731-night-eating-syndrome-nes
- Eating Disorder Hope. (n.d.). Anorexia death rate. https://www.eatingdisorderhope.com/information/anorexia/anorexia-death-rate
- Fairburn, C. G. (n.d.). A description of CBT-E. https://www.cbte.co/what-is-cbte/a-description-of-cbt-e/
- InsideOut Institute. (n.d.). DSM-5 diagnostic criteria for eating disorders. https://insideoutinstitute.org.au/resource-library/dsm-5-diagnostic-criteria-for-eating-disorders
- International Journal of Indian Psychology. (2023). Eating disorder-related research in Indian populations. https://ijip.in/wp-content/uploads/2023/04/18.01.213.20231101.pdf
- Mayo Clinic. (n.d.). Anorexia nervosa: Symptoms and causes. https://www.mayoclinic.org/diseases-conditions/anorexia-nervosa/symptoms-causes/syc-20353591
- Mayo Clinic. (n.d.). Bulimia nervosa: Symptoms and causes. https://www.mayoclinic.org/diseases-conditions/bulimia/symptoms-causes/syc-20353615
- Mental Health UK. (n.d.). Causes of eating disorders. https://mentalhealth-uk.org/help-and-information/conditions/eating-disorders/causes/
- National Eating Disorders Association. (n.d.). Eating disorder statistics. https://www.nationaleatingdisorders.org/statistics/
- National Institutes of Health. (2013). Genetics of eating disorders. https://pmc.ncbi.nlm.nih.gov/articles/PMC3599773/
- National Institutes of Health. (2023). Eating disorders overview. https://www.ncbi.nlm.nih.gov/books/NBK567717/
- National Institutes of Health. (2024). Recent research on eating disorders. https://pmc.ncbi.nlm.nih.gov/articles/PMC12457094/
- SCOFF Questionnaire. (n.d.). MDCalc. https://www.mdcalc.com/calc/10524/sick-control-one-fat-food-scoff-questionnaire
- Tele-MANAS. (n.d.). Tele Mental Health Assistance and Networking Across States. https://telemanas.mohfw.gov.in/home
- University of Western Australia. (2026, January 12). Why eating disorders are more common among LGBTQIA+ people and what can help. https://www.uwa.edu.au/news/article/2026/january/why-eating-disorders-are-more-common-among-lgbtqia-people-and-what-can-help
- WebMD. (n.d.). Orthorexia. https://www.webmd.com/mental-health/eating-disorders/what-is-orthorexia
- Wikipedia contributors. (n.d.). Body mass index. In Wikipedia, The Free Encyclopedia. Retrieved April 17, 2026, from https://en.wikipedia.org/wiki/Body_mass_index