
.png)

Mental Health Concerns
Insomnia & Sleep Issues: Meaning, Causes, Symptoms & How to Cure It (India 2026)

.png)
Written by
Aarohi Parakh,
Psychologist and Content Writer

Reviewed by
Sanjana Sivaram,
Psychologist and Clinical Content Head






Introductions
Rohan is a 34-year-old project manager at a Bengaluru edtech firm. He has been awake at 2:47 AM, 3:12 AM, and 4:05 AM for the past eleven days. He knows these times precisely because he checks his phone each time he wakes, which makes getting back to sleep harder, which he also knows. He lies in the dark, running the list of tomorrow's tasks. He tells himself he will catch up on the weekend. He never does.
His wife thinks he is stressed. His manager noticed he made an unusual error in a client document last week. His GP prescribed a short course of clonazepam to help him relax and facilitate sleep. Nobody mentioned CBT-I. Nobody asked about sleep hygiene. Nobody said the word insomnia.
Rohan is one of the estimated ~30% of Indian adults experiencing insomnia symptoms. He is one of the most predictable patients in any primary care clinic, and among the least well served. This guide covers insomnia meaning, types, symptoms, causes, and evidence-based treatment, written for the Indian context where the triggers, cultural attitudes, and available care all look different from Western clinical literature.
What is Insomnia? Meaning and Definition
Insomnia meaning: insomnia is a sleep disorder characterised by persistent difficulty falling asleep, staying asleep, or achieving restorative sleep, despite having adequate time and opportunity for sleep, causing significant daytime impairment. The defining criterion is that second part. Many people have nights of poor sleep. Insomnia is diagnosed when poor sleep consistently impairs daytime functioning.
The World Health Organization classifies insomnia under sleep-wake disorders in the ICD-11. The relevant code is 7A00-7A0Z (Insomnia disorders), which covers ongoing difficulties with falling asleep, staying asleep, or waking too early, along with daytime distress.
In the DSM-5-TR, it is called Insomnia Disorder, defined by poor sleep quality or quantity occurring at least three nights per week for at least three months, and causing noticeable distress or problems in daily functioning.
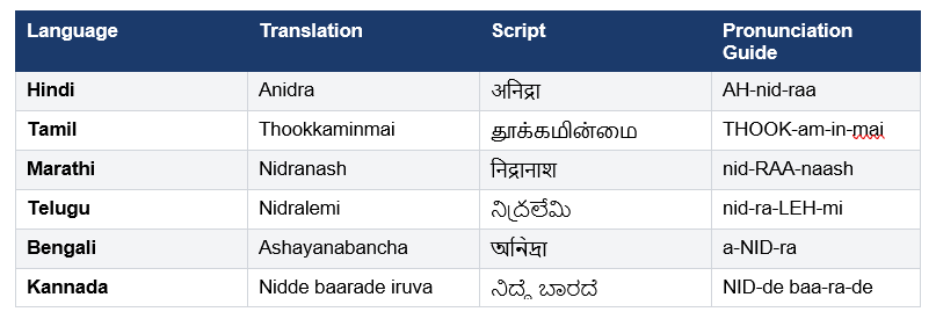
Insomnia Meaning in Indian Languages
💡Pro-Tip: India's insomnia rates are significantly underreported, not because it's rare, but because it's normalised. Cultural beliefs like “sleep = laziness” and the glorification of hustle and constant productivity make chronic sleep deprivation seem acceptable, even admirable. Many people take pride in “managing on less sleep,” without recognising the cost. However, the ICD-11 diagnosis requires not just poor sleep but measurable daytime impairment. If your poor sleep is affecting your concentration, mood, or work performance, it has already crossed the clinical threshold.
Types of Insomnia
Not all insomnia present in the same way. Clinically, insomnia is understood based on duration (short-term vs chronic), and sleep pattern difficulty (falling asleep, staying asleep, early waking). The type of insomnia determines both the likely cause and the most effective treatment approach. Treating chronic insomnia with the same strategies used for acute insomnia produces limited results.
Based on Duration
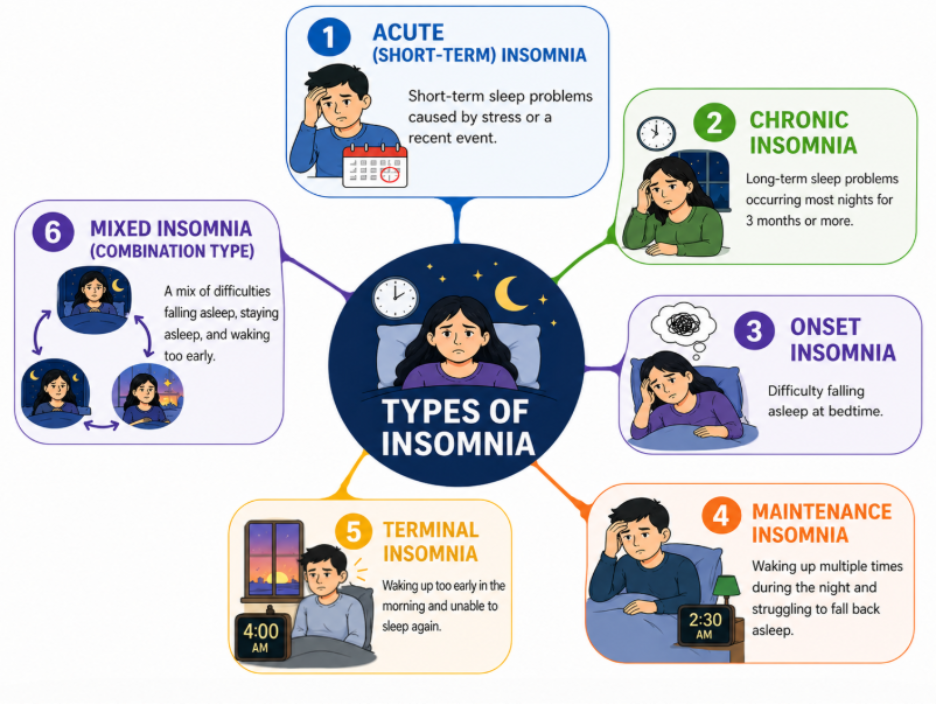
1. Acute (Short-Term) Insomnia
- Lasts a few days to a few weeks, typically linked to a specific stressor
- Usually resolves once the stressor passes
- Common causes: exams, work pressure, travel, loss, festival schedule disruption
- Example: A college student in Mumbai can’t sleep during board exams but sleep returns to normal afterward
2. Chronic Insomnia (Insomnia Disorder)
- Occurs at least 3 nights per week for 3 months or more
- Often associated with daytime impairment and needs professional support
- Common causes: Unaddressed anxiety, depression, chronic pain, shift work, prolonged stress
- Example: A call centre employee on night shifts struggles with sleep for months and feels constantly fatigued
Based on Sleep Pattern (Clinical Specifiers)
3. Onset Insomnia (Difficulty Falling Asleep)
- Trouble falling asleep despite feeling tired
- Mind feels “active” at bedtime
- Common causes: overthinking, anxiety, late-night phone use
- Example: Someone scrolls Instagram or replays conversations in their head and takes 1–2 hours to fall asleep
4. Maintenance Insomnia (Frequent Night Awakenings)
- Waking up multiple times during the night
- Difficulty going back to sleep
- Common causes: depression, chronic pain, menopause, sleep apnea
- Example: A middle-aged adult wakes up several times at night due to body pain or discomfort and feels unrefreshed in the morning
5. Terminal Insomnia (Early Morning Awakening)
- Waking up very early (around 3–5 AM) and unable to sleep again
- Often linked to mood changes
- Common causes: classic sign of clinical depression, high stress,
- Example: A person wakes at 4 AM daily with low mood and racing thoughts about life problems
6. Mixed Insomnia (Combination Type)
- Combination of onset, maintenance, and early waking difficulties
- Symptoms may change over time rather than staying fixed
- Not a formal diagnosis, but commonly used to describe real-world sleep patterns
- Common causes: overlapping stress, anxiety, irregular routines, lifestyle factors
- Example: A working professional falls asleep late due to overthinking, wakes up once or twice during the night, and then wakes early before the alarm feeling unrefreshed
Note: Most people with insomnia do not fit into just one category; symptoms often overlap or shift over time, which is why “mixed insomnia” is commonly seen in practice.
India Focus: Indian students preparing for JEE, NEET, and UPSC face a predictable seasonal pattern of acute insomnia during intensive study periods. The cultural expectation to study through the night compounds this: cramming at 1 AM suppresses melatonin, disrupts the sleep-wake cycle, and produces fatigue that directly impairs retention the next day. Sleep is not the enemy of exam performance. Sleep deprivation is.
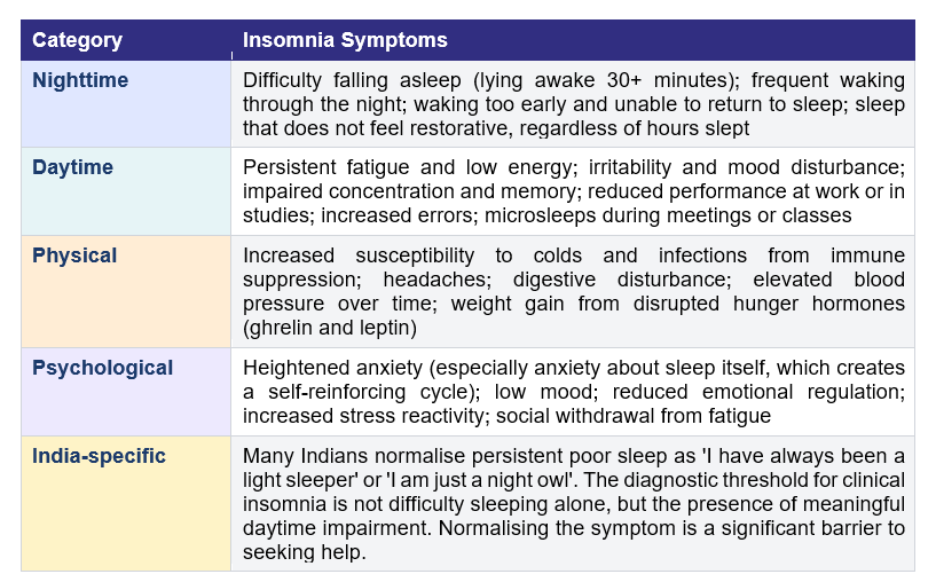
Insomnia Symptoms: How to Know If You Have Insomnia
Insomnia symptoms are not limited to the night. The daytime consequences of poor sleep are both the diagnostic requirement and, in many cases, the more disabling part of the condition. For a clinical diagnosis, these symptoms typically need to persist for at least 3 months (occurring multiple nights per week) and be associated with noticeable daytime impairment.
7 Signs You May Have Insomnia: A Self-Check
- You take more than 30 minutes to fall asleep on most nights
- You wake frequently during the night and struggle to return to sleep
- You wake 1-2 hours earlier than intended and cannot fall back asleep
- You feel unrefreshed even after 7-8 hours in bed
- You feel meaningfully tired, irritable, or foggy during the day
- Your performance at work, college, or in daily tasks is affected by tiredness
- This has been happening at least 3 nights per week for more than a month
Disclaimer: This checklist can be used for personal reflection on insomnia symptoms and is not a diagnostic tool. If four or more of these apply to you, a professional assessment is warranted.
When to Seek Professional Help for Insomnia
Even if you are unsure about a diagnosis, certain signs indicate that self-help alone may not be enough, and professional support is important.
- Sleep problems persist despite basic changes
You have tried improving your sleep routine (reducing screen time, fixing bedtime, limiting caffeine), but sleep has not improved
- Daytime functioning is clearly affected
Ongoing fatigue is impacting your work, studies, memory, mood, or safety (for example, feeling drowsy while travelling or working)
- Sleep anxiety or frustration is increasing
You feel stressed about not sleeping, or bedtime itself has become a source of worry
- Mental or physical health concerns are present
Symptoms of anxiety, low mood, chronic pain, thyroid issues, or other health conditions are affecting your sleep
- You rely on substances to sleep
Regular use of alcohol, nicotine, or sleep medications without medical guidance
- Sleep pattern is highly irregular
Frequent night shifts, jet lag, or inconsistent routines are disrupting your body clock
🚨 Red Flags: Seek Immediate / Urgent Help
- Suicidal thoughts or feelings of hopelessness
- Severe functional impairment
(e.g., unable to carry out daily responsibilities, frequent near-miss accidents, extreme exhaustion)
- Suspected sleep apnea
(loud snoring, gasping/choking during sleep, observed breathing pauses, waking unrefreshed despite adequate time in bed)
Clinical Note: If symptoms are occurring ≥3 nights per week for 3 months or more with daytime impairment, it meets the threshold for insomnia disorder and warrants professional evaluation.
Why early help matters
Early intervention can prevent short-term sleep problems from becoming chronic. Evidence-based treatments like CBT-I (Cognitive Behavioural Therapy for Insomnia) are highly effective and do not rely on long-term medication.
Where to seek help in India
- Tele MANAS: 14416 (free, 24/7 mental health helpline)
- EAP counselling services (if available through your workplace)
- Clinical psychologists, psychiatrists, or sleep specialists
Important to Note: Chronic sleep deprivation is not just an inconvenience. A large-scale study published in Sleep journal found that consistently sleeping fewer than 6 hours increases the risk of depression, obesity by 45-55%, and type 2 diabetes significantly. In India, where lifestyle diseases are already rising rapidly, chronic insomnia is a modifiable risk factor that deserves clinical attention, not just willpower.
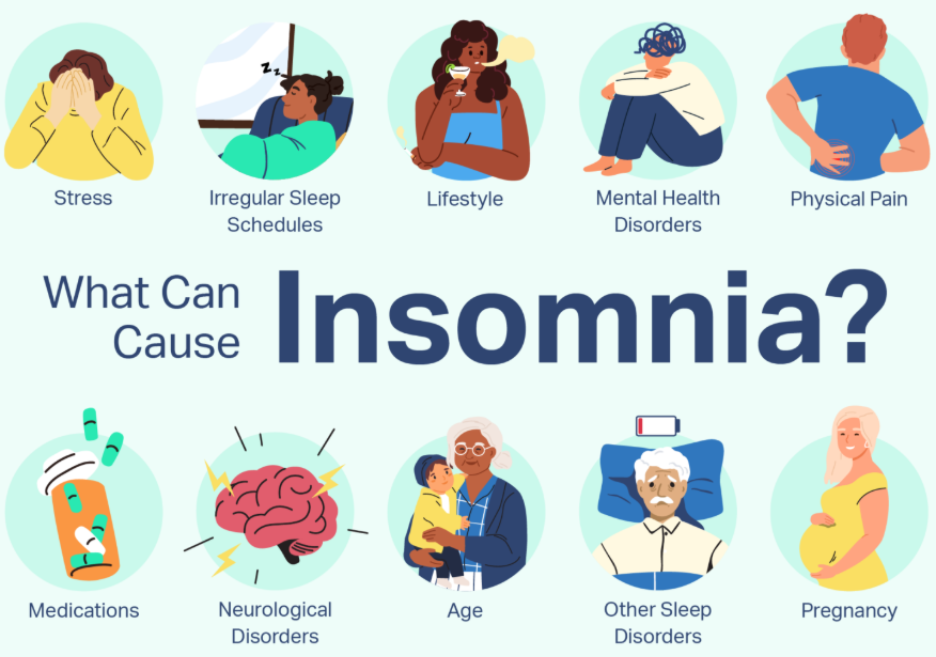
What Causes Insomnia? Triggers and Risk Factors in India
Insomnia causes are rarely singular. The most effective treatment always starts with identifying the primary driver, because no sleep intervention works well if the root cause remains unaddressed.
Psychological Causes (Most Common)
Insomnia is closely linked to mental health disorders like anxiety, depression, and PTSD. Studies indicate that about 50% of people with chronic insomnia also have at least one coexisting mental health condition.
Anxiety is the leading cause of onset insomnia in India. The hyperarousal state of anxiety, characterised by a racing mind, physical tension, and an inability to regulate, is the physiological opposite of sleep onset. Depression drives maintenance and terminal insomnia. PTSD produces nightmares and hyper-vigilant night waking.
For a detailed guide to anxiety, see our resource on anxiety: meaning, symptoms and how to overcome it.
Biological Causes
- Family history (genetics): Insomnia and other sleep-related issues often run in families, suggesting a genetic component. Specific inherited traits or predispositions may affect sleep patterns.
- Brain activity and chemistry: People with insomnia may experience heightened brain activity, making it harder to relax and fall asleep. Differences in brain chemistry and signalling pathways that regulate sleep could also play a role.
- Hormone changes: Pregnancy and menopause can affect your sleep.
Physiological and Cognitive Arousal (Maintaining Factor)
Even after the original trigger fades, insomnia often continues because of ongoing hyperarousal:
- Physiological arousal: The body remains in a “switched on” state, with elevated heart rate, muscle tension, and increased cortisol, making it difficult to transition into sleep. The nervous system does not fully downregulate at night.
- Cognitive arousal: The mind stays active at bedtime, with overthinking, worry about sleep, replaying events, or clock-watching. This creates a cycle where trying to sleep increases alertness.
Over time, the bed itself can become associated with wakefulness (conditioned arousal), which is why insomnia often persists even when the initial stressor is no longer present.
Lifestyle and Behavioural Causes
- Blue light exposure from phones, tablets, and laptops suppresses melatonin for up to 2 hours after exposure; using your phone in bed at midnight has a measurable biological impact
- Irregular sleep schedules: no consistent bedtime or wake time undermines the circadian rhythm, which requires regularity to function
- Caffeine consumption: chai and coffee consumed after 2-3 PM remain biologically active through the night for most adults
- Evening alcohol: alcohol induces initial drowsiness then causes rebound arousal in the second half of the night, producing fragmented and unrestorative sleep
- Daytime napping: napping after 3 PM reduces sleep drive at night; in India's post-lunch rest culture this is a common and underrecognised contributor
- Life circumstances: Stressful events, such as job loss, financial difficulties, or personal loss, often contribute to insomnia. While these factors might not directly cause insomnia, they can disrupt sleep patterns and increase the likelihood of insomnia.
- Medical conditions: Temporary illnesses (like COVID-19 or injuries) and chronic conditions (like chronic pain or Parkinson’s disease) can lead to insomnia.
- Life changes: Temporary changes like jet lag, sleeping in unfamiliar settings, or adjusting to a new work schedule (e.g., shift work) can disrupt sleep. Long-term life changes, such as moving or starting a new job, can also impact sleep routines.
India-Specific Triggers
- India’s large IT and BPO workforce includes a substantial number of night-shift employees, many of whom experience circadian rhythm disruption and insomnia-related symptoms, with studies showing high rates of sleep problems in this population. Rotating shifts disrupt the body clock in ways that are not simply fixed by sleeping at a different time: melatonin secretion, cortisol rhythms, and core body temperature cycles all require consistent light-dark cues to function normally.
- Indian summers create an additional environmental insomnia driver that is rarely discussed: room temperatures above 26-28 degrees Celsius prevent the core body temperature from dropping, required for deep sleep onset. Households without air conditioning in Delhi, Mumbai, and other high-temperature cities experience predictable seasonal insomnia spikes from April to June that are not primarily psychological.
- Financial stress following India's agricultural debt crisis, the urban cost-of-living pressure on young professionals, and post-2023 tech layoff anxiety are all active insomnia drivers in the Indian population.
For further information on the relationship between burnout and sleep, see our guide on burnout: meaning, symptoms and how to recover.
How to Cure Insomnia: Self-Care, CBT-I and Medical Treatment
The 2-minute military sleep method, popularised online, combines progressive relaxation with breath focus and is supported by some evidence of improved sleep-onset speed. It is a useful technique. It is not, however, a treatment for chronic insomnia. Effective treatment for insomnia depends on the cause, duration, and severity of symptoms. In most cases, non-medication approaches are recommended first, especially for long-term sleep problems. What follows below is the full spectrum, from immediate self-care to clinical intervention.
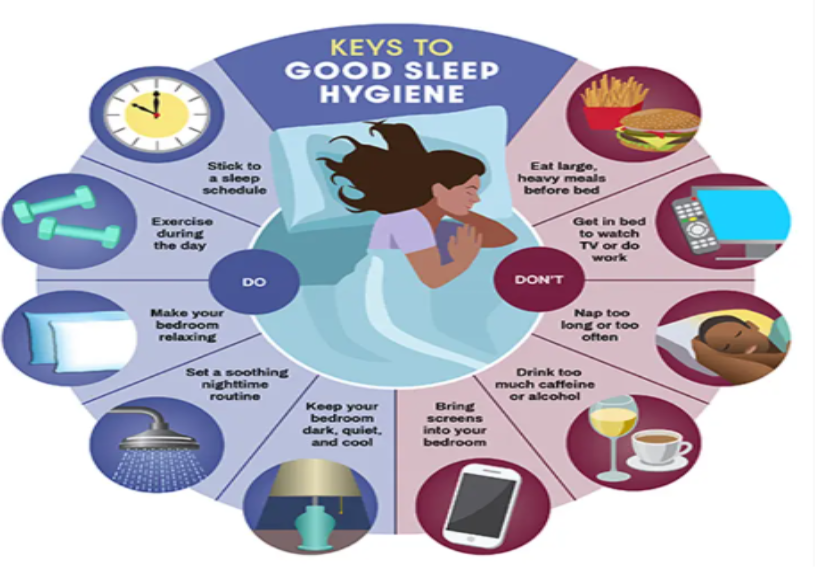
Insomnia Self-Care: The 10 Sleep Hygiene Rules (India-Adapted)
Sleep hygiene is not just advice to 'relax'. These are evidence-based behavioural changes that directly affect the neurological and hormonal systems that govern sleep. The list below is specifically adapted for Indian cultural and environmental contexts.
- Keep a consistent wake-up time, even on weekends and festival days. This is the single most powerful sleep hygiene intervention. Your biological clock anchors to your waking time, not your bedtime.
- Keep the bedroom dark and cool. Room temperature below 24°C significantly improves sleep onset for most Indian adults, particularly during the warmer months. Blackout curtains matter for urban light pollution.
- No screen time 60 minutes before bed. Phones, tablets, and laptops emit blue-spectrum light that suppresses melatonin secretion. This is not just advice; it is evidence-based: the effect is measurable within 15 minutes of exposure.
- No caffeine after 2-3 PM. Chai and coffee have a half-life of 5-6 hours in the body. If you drink chai at 5 PM, half of it is still active at 11 PM when you are trying to sleep.
- Avoid large evening meals within 2-3 hours of bedtime. India's late dinner culture (8-10 PM meals) is a genuine risk factor for insomnia for many people. Digestion and deep sleep compete for time.
- Build a 10-minute wind-down routine. The same actions in the same order each night (wash face, read a physical book, dim lights) signal to your nervous system that sleep is coming. Consistency is what makes it work.
- Avoid naps after 3 PM. A 20-minute nap before 3 PM is restorative. A 45-minute nap at 5 PM will reduce your sleep drive at 11 PM by an equivalent amount. In India, the post-lunch rest culture can directly worsen night insomnia.
- Get 20-30 minutes of morning sunlight. Natural morning light resets the circadian clock and improves sleep quality that night. A morning walk does double duty.
- Use the bed for sleep only. If you work from bed (extremely common in India's hybrid work culture), your brain learns to associate the bed with alertness. This is one of the hardest habits to break and one of the most impactful.
- If you cannot sleep after 20 minutes, leave the bed. Lying awake reinforces conditioned wakefulness. Go to another room, do something calm in dim light, and return only when sleepy. This feels counterintuitive but is clinically proven.
💡Pro-Tip: The most common sleep hygiene mistake Indians make is focusing on bedtime rather than wake time. CBT-I research consistently shows that anchoring your wake time (same time every day, even weekends, even after a bad night) is the highest-leverage single change. Bedtime will naturally stabilise once the wake time is consistent. Do this for two weeks before evaluating anything else.
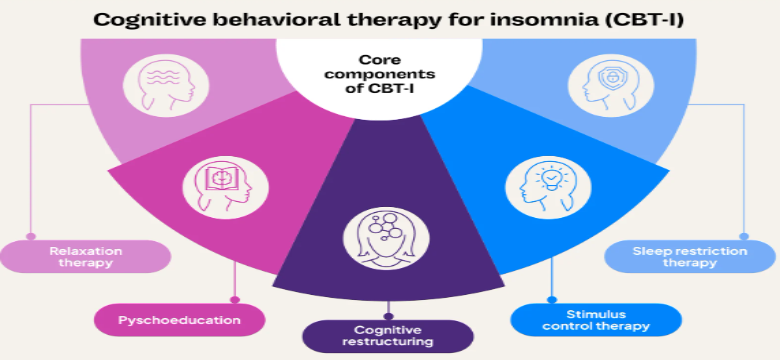
CBT-I (Cognitive Behavioural Therapy for Insomnia) — Gold Standard
Cognitive Behavioural Therapy for Insomnia (CBT-I) is the most evidence-based treatment for chronic insomnia and is more effective than medication in the long term, without dependency risks. The American Academy of Sleep Medicine and the National Sleep Foundation recommend CBT-I as the first-line treatment.
CBT-I is typically delivered over 6–8 sessions and includes:
- Sleep restriction therapy — reducing time in bed to rebuild sleep drive
- Stimulus control — associating the bed only with sleep
- Sleep hygiene education — improving daily habits
- Relaxation training — calming the body and mind
- Cognitive therapy — addressing unhelpful thoughts about sleep
Access in India: Available through trained clinical psychologists and government-supported centres such as the NIMHANS Sleep Disorders Clinic for specialised care.
Behavioural & Lifestyle Interventions
These are often part of CBT-I but can also be started independently:
- Sleep restriction therapy
Useful for chronic insomnia, but should ideally be done under guidance
- Stimulus control
Over time, this reduces frustration and “conditioned wakefulness”
- Yoga nidra and pranayama
Effective for mild to moderate insomnia and prevention; widely accessible in India
Medications (Short-Term & Case-Specific)
Medication is not first-line for chronic insomnia, but may be used in specific situations:
- Melatonin (over-the-counter)
- Useful for circadian rhythm issues, jet lag, shift work
- Typical dose: 0.5–5 mg
- Generally safe for short-term use
Variation in response: Not everyone responds the same way. Some people notice improved sleep onset, while others experience minimal benefit. Timing, dose, individual biology, and the underlying cause of insomnia all influence effectiveness.
Important considerations:
- Not a long-term standalone solution for chronic insomnia
- Works best when combined with behavioural strategies (sleep routine, light exposure, CBT-I principles)
- If sleep problems persist, it should be used under professional guidance rather than self-managed long term
- Prescription sleep medications
- Used for acute insomnia or severe distress
- Includes benzodiazepines and Z-drugs
- Require psychiatrist supervision due to dependency risk
- Low-dose antidepressants
- Used when insomnia occurs alongside anxiety or depression
- Prescribed by a psychiatrist
How to Choose the Right Treatment
- Short-term insomnia: lifestyle changes + short-term support
- Chronic insomnia: CBT-I is the most effective approach
- Insomnia with mental health concerns: combined therapy + medication may be needed
Important to Note: Sleeping tablets do not treat insomnia. They treat the symptom of not sleeping, while the underlying cause continues. Benzodiazepines and Z-drugs (zolpidem, zopiclone) can lead to dependence, especially with prolonged or unsupervised use. If you are currently on sleeping tablets and want to taper, do not stop abruptly: speak to your prescribing doctor about a structured reduction plan.
Insomnia and Mental Health: The Bidirectional Link
Insomnia and mental health have a direct bidirectional relationship: Insomnia is a sleep-wake disorder closely linked to mental health conditions. This is the most commonly missed clinical insight in Indian primary care, where insomnia is frequently treated with a sleep medication without any assessment of the psychological component.
- Insomnia and anxiety: the hyperarousal state that defines anxiety is the physiological opposite of sleep onset. Racing thoughts, physical tension, and an inability to downregulate prevent the cognitive quieting that sleep requires. Treating anxiety significantly improves insomnia in most cases.
- Insomnia and depression: early morning awakening (terminal insomnia) is a classic diagnostic indicator of clinical depression. It is often the first symptom that presents to a GP. Treating the depression is the primary intervention; sleep usually improves within 2-4 weeks of effective antidepressant treatment.
- Insomnia and stress: acute stress disrupts sleep through cortisol elevation and sympathetic nervous system activation. Chronic insomnia then worsens stress tolerance, reduces emotional regulation capacity, and increases cortisol reactivity. The cycle is self-reinforcing without deliberate interruption.
- Research led by Jamie Zeitzer at Stanford Medicine suggests that sleep timing matters as much as sleep duration for mental health. In a large U.K. study of nearly 75,000 people, individuals who slept and woke earlier had lower risks of depression and anxiety, even if they naturally preferred staying up late. Interestingly, this goes against the idea that simply following one’s natural sleep preference (whether you’re more of a “night person” or “morning person”) is always healthiest. Late sleepers showed higher mental health risks regardless of their preference.
One explanation is the concept of “mind after midnight”: late-night hours are linked to poorer decision-making, reduced social structure, and increased emotional vulnerability, which may negatively impact mental health over time.
Sleep Disorders Beyond Insomnia: A Quick Guide
Insomnia is the most common sleep disorder, but several others deserve mention because they are frequently underdiagnosed in India and are sometimes the actual cause of what presents as insomnia.
- Sleep apnea: repeated breathing interruptions during sleep, often unnoticed by the sleeper but reported by partners as snoring or gasping. More common in overweight adults and significantly more prevalent in India than clinical detection rates suggest. Requires polysomnography (overnight sleep study) for diagnosis; treated with CPAP machine or weight management.
- Restless Leg Syndrome (RLS): an uncomfortable urge to move the legs, typically worsening in the evening and disrupting sleep onset. More common in pregnancy and in people with anaemia, both of which are highly prevalent in India. Iron supplementation often resolves it.
- Sleep paralysis: temporary inability to move upon waking, often accompanied by hallucinations. High search volume in India because it is frequently misinterpreted as a supernatural experience. It is a REM sleep intrusion phenomenon, not a spiritual event, and is benign in most cases.
- Shift work sleep disorder: chronic circadian misalignment in India's large number of night-shift workers. The body never fully adapts to overnight schedules. CBT-I adapted for shift workers and strategic melatonin use are the primary interventions.
- Narcolepsy: rare, but often undiagnosed for years in India. Characterised by excessive daytime sleepiness, sudden muscle weakness (cataplexy), and disturbed night sleep. Requires neurological assessment.
- Delayed sleep phase syndrome: Characterised by falling sleep at least two hours after one’s desired bedtime and having difficulty waking up for school or work.
If insomnia persists for three or more months despite consistent sleep hygiene changes, or if your partner reports snoring, breathing pauses, or leg movements during sleep, see a sleep specialist. In India, NIMHANS and AIIMS both have specialist sleep medicine clinics. If you are unsure where to begin, you can also reach out to your EAP counselling helpline (if available through your workplace) or Tele MANAS at 14416 for structured guidance, next steps, or referral pathways.
A Final Word
Rohan eventually saw a clinical psychologist trained in CBT-I. He did not receive more medication. He received structured sessions, a consistent wake time, and a clear understanding of how his sleep patterns were being maintained. Within six weeks, he was sleeping through the night most days. What helped him most was realising that his struggle was a common and treatable problem.
In India, insomnia is often not treated effectively because it is not fully understood. It is still frequently addressed with short-term medication and general advice to “stress less.” This is not enough for the many adults whose sleep, mood, and daily functioning are affected, despite the availability of effective, evidence-based treatments.
If you recognise yourself in this guide, start with small steps. Track your sleep, set a consistent wake time, and seek professional support. You can call Tele MANAS (14416) for free mental health support and referrals. If your organisation offers an Employee Assistance Programme (EAP) such as 1to1help, confidential counselling is also available and can connect you to trained professionals.
You do not have to keep waking up in the middle of the night. Help is available, and sleep can improve.
Downloadable Resources
- Sleep Diary (National Sleep Foundation): 7-day printable sleep diary to track patterns, identify triggers, and measure CBT-I progress :https://www.thensf.org/wp-content/uploads/2021/02/NSF-Sleep-Diary-Rev-2-2021.pdf
- CBT-I Coach App: Structured CBT-I programme; sleep diary, sleep restriction guide, thought records; evidence-based: Available free on iOS and Android; search 'CBT-I Coach'
- Yoga Nidra (Art of Living): Guided 20-30 minute deep relaxation; proven to reduce sleep onset time: https://www.youtube.com/watch?v=RcXemRLVW1Q
💡Pro-Tip: Start with two things this week: download and fill in a 7-day sleep diary from the National Sleep Foundation, and set a consistent wake time you will use every day for the next 14 days. These two actions alone will give you the data you need and begin the biological reset on which CBT-I is built. Do not wait until you have read everything about insomnia to start improving your sleep.
FAQs
Q1. What is insomnia and what does it mean?
Insomnia is a sleep disorder characterised by persistent difficulty falling asleep, staying asleep, or achieving restorative sleep, despite having adequate opportunity, causing meaningful daytime impairment. In Hindi, insomnia meaning in Hindi is "अनिद्रा" (anidra). The defining feature is not just poor sleep at night but significant daytime effects: fatigue, difficulty concentrating, mood disturbances, or reduced performance. Insomnia affects an estimated ~30% of Indian adults, making it among the most common health conditions in the country. Chronic insomnia (3+ nights per week for 3+ months) requires professional attention and responds well to CBT-I treatment.
Q2. What causes insomnia?
Insomnia causes are most commonly psychological: anxiety, depression, PTSD, and chronic stress are the leading drivers. Biological causes including family genetics and changes in brain chemistry or hormonal changes. Behavioural causes including screen use before bed, irregular schedules, caffeine after 2 PM, and daytime napping are also significant. In India, specific triggers include competitive exam pressure, night-shift IT and BPO work, summer heat disrupting sleep onset temperature, and financial stress. Medical causes include chronic pain, thyroid disorders, GERD, and certain medications. Identifying the root cause is essential because insomnia treatments work best when they address the specific driver rather than only the symptom of not sleeping.
Q3. How to cure insomnia quickly at home?
The most immediately actionable step is to set a consistent wake time and maintain it for 14 days. This single change produces measurable improvement in sleep quality faster than any other self-care intervention. Complementary steps: no screens 60 minutes before bed, no caffeine after 2 PM, room temperature below 24°C where possible, and a 10-minute wind-down routine. The 'military sleep method' circulating online involves progressive muscle relaxation and breath focus over approximately 2 minutes and helps some people fall asleep faster. For how to cure insomnia more durably, CBT-I is the evidence-based gold standard and is significantly more effective than medication for chronic insomnia.
Q4. Is insomnia a mental health problem?
Yes. Insomnia is classified as a mental health and neurological condition under both ICD-11 and DSM-5 TR. It frequently co-occurs with anxiety disorders and depression, and each worsens the other in a bidirectional cycle. Chronic insomnia increases the risk of clinical depression threefold and significantly worsens anxiety. In India, insomnia is frequently dismissed as 'just stress' and treated only with sleeping tablets, missing the psychological component entirely. Effective treatment addresses both sleep and mental health simultaneously, which is why CBT-I, which targets both, produces more lasting results than medication alone.
Q5. What is CBT-I and is it available in India?
CBT-I (Cognitive Behavioural Therapy for Insomnia) is the gold-standard treatment for chronic insomnia, recommended above medication by the American Academy of Sleep Medicine. It involves sleep restriction, stimulus control, sleep hygiene education, relaxation training, and cognitive therapy targeting unhelpful beliefs about sleep. It typically takes 6-8 sessions and produces lasting improvements. In India, CBT-I trained therapists are available in major cities and through government-supported institutions such as the NIMHANS and AIIMS, which offer specialised sleep services.
You can also call Tele MANAS (14416) for free mental health support and guidance to appropriate services in your language. If your workplace provides an Employee Assistance Program (EAP), confidential counselling is available and can help connect you to a CBT-I trained professional.
The CBT-i Coach app (free on iOS and Android) provides a structured self-guided programme that can be used alongside therapy.
Q6. What medicines are available for insomnia in India?
In India, melatonin (0.5-5mg) is available over the counter and is safe for short-term use to reset the circadian clock. Antihistamines such as diphenhydramine are also OTC options but develop tolerance quickly. Prescription options include benzodiazepines (e.g., clonazepam) and Z-drugs (e.g., zolpidem), both carrying significant dependency risk with regular use beyond 2-4 weeks. Low-dose antidepressants are sometimes prescribed for insomnia with comorbid depression. Ashwagandha has mild clinical evidence for improving sleep quality and is widely available. Always consult a doctor before starting insomnia treatment medication.
Q7: How much sleep do I actually need?
The National Sleep Foundation recommends 7-9 hours for adults (18-64 years), 8-10 hours for teenagers, and 9-11 hours for school-age children. Older adults (65+) need 7-8 hours. Individual variation exists: some adults function well on 6.5 hours, others need 9. Quality matters as much as quantity: uninterrupted, deep sleep is more restorative than long, fragmented sleep. In India, cultural attitudes frequently normalise insufficient sleep as productivity. Consistently sleeping fewer than 6 hours is associated with significantly increased risks of obesity, type 2 diabetes, cardiovascular disease, and depression.
References
- American Academy of Sleep Medicine. (n.d.). Cognitive behavioral therapy for insomnia. Sleep Foundation. https://www.sleepfoundation.org/insomnia/treatment/cognitive-behavioral-therapy-insomnia
- Best Practice BMJ. (n.d.). Insomnia. https://bestpractice.bmj.com/topics/en-gb/227
- Cleveland Clinic. (n.d.). Insomnia. https://my.clevelandclinic.org/health/diseases/12119-insomnia
- Cleveland Clinic. (n.d.). Sleep disorders. https://my.clevelandclinic.org/health/diseases/11429-sleep-disorders
- Cleveland Clinic. (n.d.). Depression. https://my.clevelandclinic.org/health/diseases/9290-depression
- Cleveland Clinic. (n.d.). Chronic pain. https://my.clevelandclinic.org/health/diseases/4798-chronic-pain
- Cleveland Clinic. (n.d.). Menopause. https://my.clevelandclinic.org/health/diseases/21841-menopause
- Cleveland Clinic. (n.d.). Thyroid disease. https://my.clevelandclinic.org/health/diseases/8541-thyroid-disease
- Cleveland Clinic. (n.d.). Benzodiazepines. https://my.clevelandclinic.org/health/treatments/24570-benzodiazepines-benzos
- Cleveland Clinic. (n.d.). Cortisol. https://my.clevelandclinic.org/health/articles/22187-cortisol
- Cleveland Clinic. (n.d.). CPAP machine. https://my.clevelandclinic.org/health/treatments/22043-cpap-machine
- Cleveland Clinic. (n.d.). Cataplexy. https://my.clevelandclinic.org/health/symptoms/cataplexy
- Cleveland Clinic. (n.d.). Anemia. https://my.clevelandclinic.org/health/diseases/3929-anemia
- Fluent in Health. (n.d.). A guide to insomnia: Why can’t I fall asleep? https://fluentinhealth.com/blog/a-guide-to-insomnia-why-cant-i-fall-asleep-eB0O6mgaRRqae2R~UTl_Cg
- Fluent in Health. (n.d.). No more sleepless nights: Here’s how to get deep sleep. https://fluentinhealth.com/blog/no-more-sleepless-nights-heres-how-to-get-deep-sleep-8jZ8vrbRSn6gfFB22_7SPA
- Food and Drug Administration. (n.d.). Taking Z-drugs for insomnia? Know the risks. https://www.fda.gov/consumers/consumer-updates/taking-z-drugs-insomnia-know-risks
- Gupta, R., et al. (2017). Clinical practice guidelines for sleep disorders. Indian Psychiatric Society. https://indianpsychiatricsociety.org/wp-content/uploads/2022/05/Gupta_2017_Clinical_Practice_Guidelines_for_Sleep.pdf
- Healthline. (n.d.). Sleep hygiene. https://www.healthline.com/health/sleep-hygiene
- Hopkins Medicine. (n.d.). The effects of sleep deprivation. https://www.hopkinsmedicine.org/health/wellness-and-prevention/the-effects-of-sleep-deprivation
- Indeed. (n.d.). What is shift work? https://www.indeed.com/career-advice/finding-a-job/what-is-shift-work
- Mayo Clinic. (n.d.). Insomnia: Symptoms and causes. https://www.mayoclinic.org/diseases-conditions/insomnia/symptoms-causes/syc-20355167
- Mayo Clinic. (n.d.). Stress management. https://www.mayoclinic.org/healthy-lifestyle/stress-management/in-depth/stress/art-20046037
- Mayo Clinic. (n.d.). Sleep apnea. https://www.mayoclinic.org/diseases-conditions/sleep-apnea/symptoms-causes/syc-20377631
- Mayo Clinic. (n.d.). GERD. https://www.mayoclinic.org/diseases-conditions/gerd/symptoms-causes/syc-20361940
- Mayo Clinic. (n.d.). Melatonin side effects. https://www.mayoclinic.org/healthy-lifestyle/adult-health/expert-answers/melatonin-side-effects/faq-20057874
- Mayo Clinic. (n.d.). Post-traumatic stress disorder. https://www.mayoclinic.org/diseases-conditions/post-traumatic-stress-disorder/symptoms-causes/syc-20355967
- Mayo Clinic. (n.d.). Parkinson’s disease. https://www.mayoclinic.org/diseases-conditions/parkinsons-disease/symptoms-causes/syc-20376055
- MindTalk. (n.d.). Sleep disorder. https://www.mindtalk.in/illnesses/sleep-disorder
- National Health Service. (n.d.). Clonazepam: Common questions. https://www.nhs.uk/medicines/clonazepam/common-questions-about-clonazepam/
- National Library of Medicine. (2024). Sleep study research. https://pmc.ncbi.nlm.nih.gov/articles/PMC12482946/
- National Library of Medicine. (2019). Sleep issues in BPO workers. https://pmc.ncbi.nlm.nih.gov/articles/PMC6817959/
- Sleep Foundation. (n.d.). Types of insomnia. https://www.sleepfoundation.org/insomnia/types-of-insomnia
- Sleep Foundation. (n.d.). REM sleep. https://www.sleepfoundation.org/stages-of-sleep/rem-sleep
- Stanford News. (2025). Sleep timing and mental health research. https://news.stanford.edu/stories/2025/08/sleep-mental-health-mood-impact-science-research
- Tele MANAS. (n.d.). National tele mental health programme. https://telemanas.mohfw.gov.in/home
- Verywell Mind. (n.d.). Military sleep method. https://www.verywellmind.com/military-sleep-method-7111161
- WebMD. (n.d.). What is pranayama? https://www.webmd.com/balance/what-is-pranayama
- World Health Organization. (n.d.). ICD-11 classification of sleep disorders. https://icd.who.int/dev11/f/en#/http://id.who.int/icd/entity/274880002
- Find-A-Code. (n.d.). ICD-11 sleep disorders block. https://www.findacode.com/icd-11/block-1038292737.html
- Yoga International. (n.d.). Benefits of yoga nidra. https://yogainternational.com/article/view/5-benefits-of-yoga-nidra/
- Dr. Nalini Nagalla. (n.d.). Sleep disorders in India. https://drnalininagalla.com/blog/the-silent-pandemic-of-sleep-disorders-in-india/