
.png)

Mental Health Concerns
Mental Health in India: A Complete Guide to Understanding, Managing & Improving Your Mental Well-Being

.png)
Written by
Aarohi Parakh,
Psychologist and Content Writer

Reviewed by
Sanjana Sivaram,
Psychologist and Clinical Content Head






Introduction

Arjun is a 31-year-old project manager at a mid-sized IT firm in Pune. By most metrics, his life looks fine. He has a stable job, a supportive family, and a flat he owns. But for the past eight months, he has been waking at 3 am with a racing heart, dreading the working day before it begins. He has told no one. In his family, talking about feelings has never been normalised. At work, it could be career-limiting. He has Googled his symptoms twice and closed the tab both times.
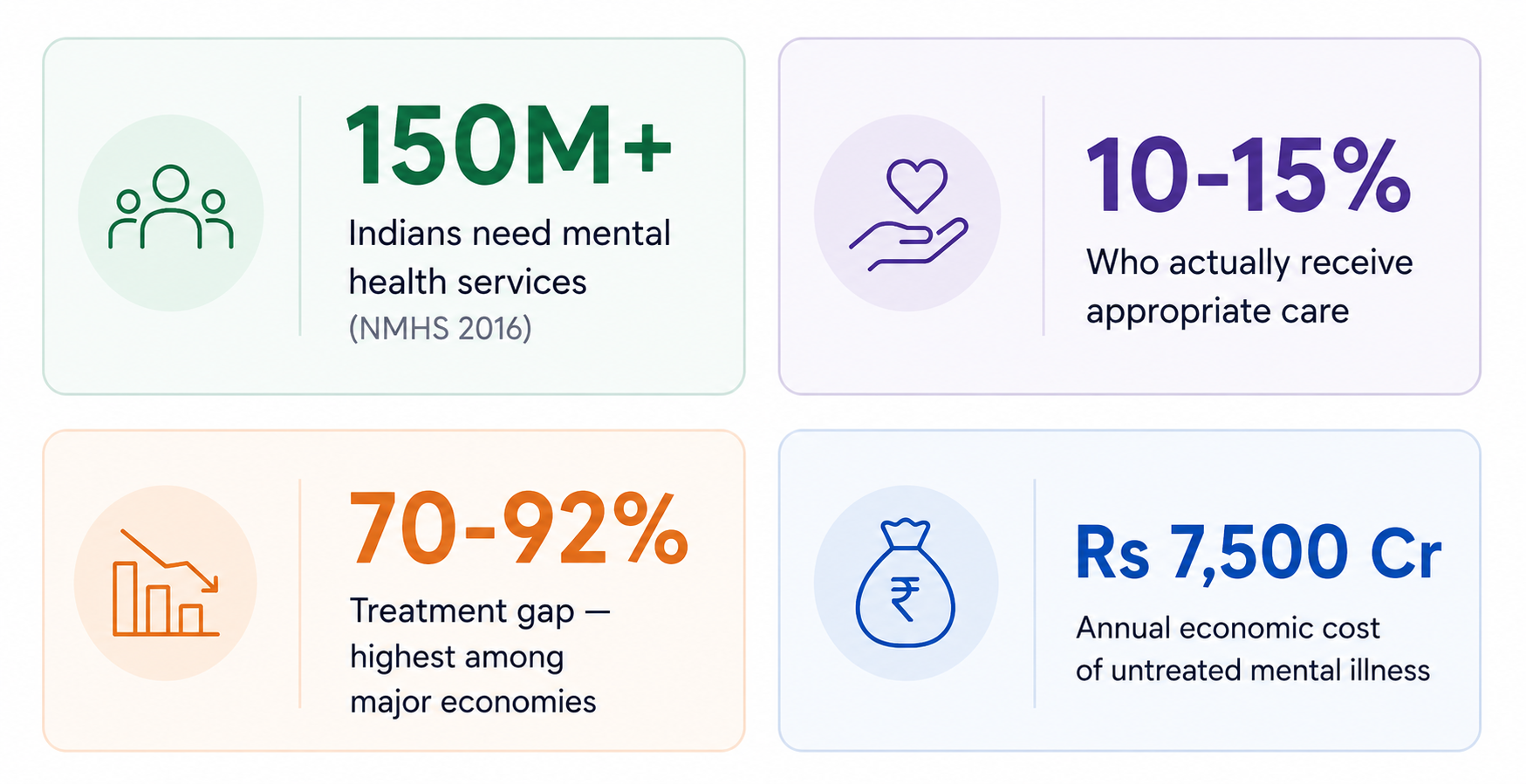
Arjun is not alone. An estimated 150 million Indians need mental health care, but only 10 to 15 percent receive it. The gap between need and access is not just a statistic. It is millions of people across every city and state who are managing distress in silence because the frameworks to understand it, the language to name it, and the resources to address it often remain inaccessible.
Mental health is not a niche concern or a Western concept that we have imbibed. It is a fundamental dimension of how we function, relate, work, and live.
This comprehensive guide covers what mental health is, how it can begin to deteriorate, what the warning signs look like, what causes it to deteriorate, and what treatments and resources are available in India today. Whether you are navigating something yourself or supporting someone you care about, this guide is a useful starting point.
What Is Mental Health? Definition, Dimensions, and Why It Matters
Mental health is defined by the World Health Organisation (WHO, 2022) as a state of well-being in which an individual realises their own potential, can cope with the normal stressors of life, can work productively, and is able to contribute to their community. Critically, the WHO definition makes clear that good mental health is not simply the absence of mental illness. It is a positive, active state.
India's Economic Survey 2024-25 expanded this framing, defining mental well-being as encompassing mental-emotional, social, cognitive, and physical capabilities. This four-dimensional understanding reflects a growing recognition that mental health is not a single variable but an interconnected system.
The Three Core Dimensions of Mental Health
Arjun’s experience from our introduction is not limited to a single symptom like disturbed sleep or anxiety. It reflects how mental health operates across three interconnected dimensions:
Emotional Health (What we feel)
In Arjun’s case, the 3 am awakenings are not random. There are moments when underlying emotions, especially anxiety, surface when the mind is no longer occupied.
During the day, people often push these feelings aside to keep functioning. But unprocessed emotions tend to find expression, often at night or during quiet moments.
👉 Emotional health refers to the ability to recognise, process, and regulate these internal states rather than becoming overwhelmed by them.
Psychological Health (How we think)
Alongside emotions, patterns of thinking shape distress.
For someone like Arjun, this may include:
- Pressure to “handle things” independently
- Fear of consequences if he opens up
- A tendency to avoid confronting what feels uncomfortable
These reflect rigid patterns of thinking and a tendency to avoid difficult emotions or situations, both of which are key aspects of psychological health.
Approaches such as Cognitive Behavioural Therapy focus on identifying and restructuring these thought patterns to build flexibility and resilience.
Social Health (How we connect)
Many people struggle to reach out for support because emotional expression does not always feel safe, comfortable, or familiar.
Arjun’s silence is not unusual. In many Indian contexts, conversations around feelings are limited, and vulnerability can feel unsafe, especially in professional spaces.
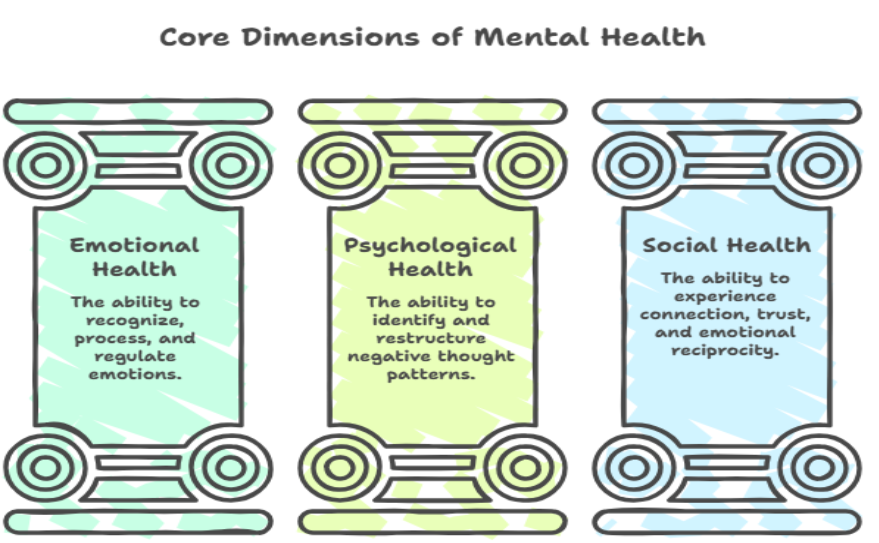
👉 Social health refers not just to having people around, but to experiencing connection, trust, and emotional reciprocity.
Arjun’s situation illustrates a broader point. When one dimension is affected, the others are often pulled in the same direction.
Mental Health vs Mental Illness: Key Differences
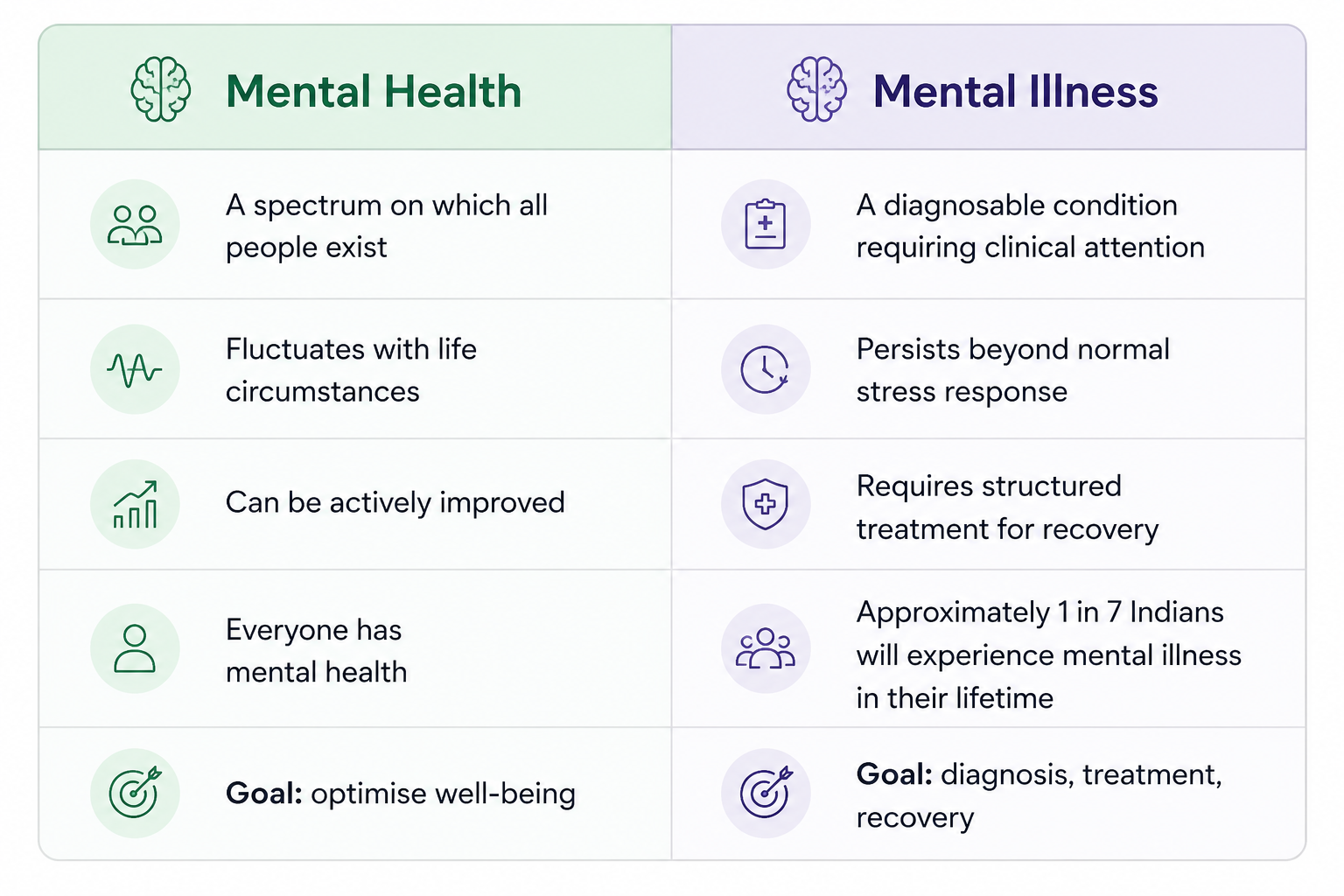
According to the National Mental Health Survey (NIMHANS 2015-16), approximately 10.6 percent of Indian adults (roughly 11 in every 100) live with a diagnosable mental disorder. The lifetime prevalence is 13.7 percent, meaning that approximately 1 in 7 Indians will experience a clinically significant mental health condition at some point in their lives.

India-specific context: Mental health in India is shaped by a distinctive set of pressures: rapid urbanisation that severs traditional social ties, the intense competition of the educational system (JEE, NEET, board exams), economic precarity, caste-related stressors, and a cultural framework that frequently pathologises help-seeking as weakness. Understanding mental health in India means understanding these specific pressures alongside universal clinical frameworks.
Mental Health in India: Key Statistics and the Treatment Gap
How Big Is the Mental Health Crisis in India?
The scale of India's mental health challenge is significant, measurable, and largely unaddressed. The following statistics draw on India's most authoritative sources.
📊 India's Mental Health Statistics at a Glance
- 150 million Indians need mental health services (National Mental Health Survey, NIMHANS 2016)
- Treatment gap of 70 to 92 percent: the proportion of people who need care but do not receive it — the highest among major global economies (Lancet Psychiatry, 2016)
- 1 in 7 Indians will experience a mental disorder in their lifetime (NIMHANS NMHS 2015-16)
- Depression affects 56 million, and anxiety affects 44 million Indians (WHO India data)
- India ranked 60th globally in youth mental health with an MHQ score of 33 vs global average of 66 (Sapien Labs 2025)
- The WHO estimates India loses USD 1.03 trillion to mental health conditions between 2012 and 2030 in lost economic output
- India has 0.75 psychiatrists per 100,000 people; the WHO recommends a minimum of 3 (WHO Atlas 2020)
A large number of people in India (70 to 92 percent, depending on the condition) who could benefit from mental health support still do not receive timely care. This is influenced by several structural and practical barriers, including:
- Limited availability of trained mental health professionals,
- Greater concentration of services in urban areas compared to rural regions
- Financial constraints and affordability concerns in private care
- Social stigma and hesitation around seeking help
- Historically lower prioritisation of mental health within healthcare systems
The economic dimension is equally significant. The WHO estimates that India will lose USD 1.03 trillion in economic output between 2012 and 2030 due to mental health conditions. Untreated depression and anxiety alone are among the leading causes of workplace absenteeism, presenteeism, and early exit from the workforce in India.
It should be noted that increased awareness, digital access, workplace support programs, and government-led initiatives are gradually improving access to mental health care across the country.
Types of Mental Health Disorders: Your Complete Sub-topic Guide
Mental health conditions are classified using two primary frameworks: the DSM-5 TR (American Psychiatric Association) and the ICD-11 (World Health Organization). Both organise conditions into categories based on symptom clusters, causes, and treatment approaches. What follows is a clinically accurate, accessible overview of the 20 most prevalent and most-searched conditions in India, with links to their dedicated full-length guides.
Mood Disorders
1. Depression
Depression is a mental health condition characterised by persistent low mood, loss of interest in activities once enjoyed, fatigue, and a range of cognitive and physical symptoms lasting at least two weeks.
Key symptom: Persistent low mood lasting more than two weeks, with reduced energy and loss of pleasure
India: Affects an estimated 56 million Indians; significantly underdiagnosed in men and the elderly
2. Bipolar Disorder
Bipolar disorder involves alternating episodes of mania (elevated mood, reduced sleep, impulsivity) and depression. It affects approximately 1 percent of the global population.
Key symptom: Extreme mood swings between elevated, energised states and episodes of deep depression
India: Prevalence estimated at 0.5 percent of the Indian population; frequently misdiagnosed as depression
3. Grief and Bereavement
Grief is the natural response to significant loss. Prolonged grief disorder occurs when acute grief does not resolve over time and becomes a clinical condition impairing daily functioning.
Key symptom: Persistent, intense longing for the deceased; difficulty accepting the loss; impaired functioning
India: Significantly underrecognised in India where grief is culturally expected to be endured privately
4. Post-partum Depression
Post-partum depression occurs in the weeks and months following childbirth and affects the mother's ability to care for herself and her child. It is distinct from normal 'baby blues'.
Key symptoms: Persistent sadness, difficulty bonding with the newborn, anxiety, and exhaustion following childbirth
India: Affects an estimated 22 percent of Indian mothers; severely underdiagnosed
Anxiety-Related Disorders
5. Anxiety Disorders
Anxiety disorders are characterised by persistent, excessive worry or fear that is disproportionate to the actual situation. They include generalised anxiety, social anxiety, panic disorder, and phobias.
Key symptom: Persistent worry, physical tension, avoidance behaviour, and impairment in daily functioning
India: Affects an estimated 44 million Indians; one of the most common but undertreated conditions
6. OCD (Obsessive-Compulsive Disorder)
OCD is characterised by recurring, unwanted thoughts (obsessions) and repetitive behaviours or mental rituals (compulsions) performed to reduce anxiety. The full form of OCD in Hindi is junooni badhyakari vikar.
Key symptom: Intrusive, unwanted thoughts followed by repetitive rituals consuming more than one hour per day
India: Affects 2 to 3.3 percent of Indians; highly treatable with Exposure and Response Prevention (ERP) therapy
7. Phobias
A phobia is an intense, persistent, irrational fear of a specific object, situation, or activity that causes significant distress or avoidance. Specific phobias are among the most treatable mental health conditions.
Key symptom: Severe anxiety or panic response to a specific feared stimulus, leading to significant avoidance
India: Affects 4 to 5 percent of the Indian population; animal and situational phobias most prevalent
8. Panic Disorder
Panic disorder involves recurrent, unexpected panic attacks: sudden surges of intense fear with physical symptoms including racing heart, breathlessness, and a sense of impending doom.
Key symptom: Recurrent unexpected panic attacks followed by persistent worry about future attacks
India: Affects 0.5 percent of Indians; frequently mistaken for cardiac events, delaying mental health treatment
9. PTSD (Post-Traumatic Stress Disorder)
PTSD develops following exposure to a traumatic event and involves intrusive memories, hypervigilance, emotional numbing, and avoidance. It can develop after any trauma: accidents, assault, natural disasters, or abuse.
Key symptom: Flashbacks, nightmares, emotional numbing, and persistent hyperarousal following a traumatic event
India: Significantly underdiagnosed in India; particularly prevalent in survivors of domestic violence and natural disasters
Psychotic and Serious Mental Disorders
10. Schizophrenia
Schizophrenia is a serious mental disorder characterised by psychosis, including hallucinations, delusions, and disorganised thinking. With appropriate treatment, most people with schizophrenia can live fulfilling lives.
Key symptom: Hallucinations (hearing voices), delusions, disorganised speech, and impaired daily functioning
India: Affects approximately 0.3 to 0.5 percent of the Indian population; accounts for a significant share of psychiatric hospital admissions
11. Personality Disorders (BPD)
Borderline Personality Disorder (BPD) involves an unstable sense of self, intense emotional responses, impulsivity, and unstable relationships. It is often misunderstood and heavily stigmatised.
Key symptom: Intense fear of abandonment, rapidly shifting moods, impulsivity, and turbulent relationships
India: Estimated prevalence of 1 to 2 percent in India; significantly underdiagnosed in the absence of specialist training
Neurodevelopmental Conditions
12. ADHD (Attention Deficit Hyperactivity Disorder)
ADHD is a neurodevelopmental condition characterised by persistent inattention, hyperactivity, and impulsivity that impairs functioning. It frequently persists into adulthood and is increasingly recognised in Indian adults.
Key symptom: Difficulty sustaining attention, impulsivity, and hyperactivity causing impairment across settings
India: Affects 5 to 8 percent of Indian children; adult ADHD significantly underdiagnosed
13. Autism Spectrum Disorder (ASD)
ASD is a neurodevelopmental condition affecting social communication and behaviour, characterised by a spectrum of presentations from mild to severe. Prevalence in India is rising as awareness and diagnostic capacity improve.
Key symptom: Differences in social communication, repetitive behaviours, and sensory sensitivities
India: Estimated prevalence of 1 in 68 children in India (Indian Pediatrics, 2024); significant diagnostic delay
Eating Disorders and Lifestyle Conditions
14. Eating Disorders
Eating disorders are serious mental health conditions involving persistent disturbances in eating behaviour and distressing thoughts about food, body weight, and body image. They include anorexia, bulimia, binge eating disorder, and ARFID.
Key symptom: Restrictive eating, binge-purge cycles, or loss-of-control eating, accompanied by intense psychological distress
India: Significantly underdiagnosed in India; rising particularly among urban youth aged 13 to 30
15. Substance Use Disorders
Substance use disorders involve a pattern of alcohol or drug use that causes clinically significant impairment. Alcohol use disorder is among the most prevalent mental health conditions in India, particularly in men.
Key symptom: Loss of control over substance use, tolerance, withdrawal, and continued use despite harm
India: Alcohol use prevalence 9.4 percent, with Indian males having a higher prevalence. (Indian Journal of Psychiatry, 2024)
16. Sleep Disorders
Sleep disorders include insomnia, sleep apnoea, and circadian rhythm disruptions. They are both causes and consequences of poor mental health, creating bidirectional reinforcing cycles.
Key symptom: Difficulty falling or staying asleep, non-restorative sleep, and daytime impairment
India: A 2025 systematic review published in the Indian Journal of Public Health found that 25.7 percent of Indians suffer from insomnia, while 37.4 percent are affected by obstructive sleep apnea (OSA). Another 10.6 percent experience restless leg syndrome, a condition that disrupts sleep cycles.
Stress, Adjustment, and Wellness-Related Conditions
17. Stress and Burnout
Chronic stress and burnout represent a spectrum from normal stress responses to clinical exhaustion states. Burnout is characterised by emotional exhaustion, cynicism, and reduced professional efficacy.
Key symptom: Emotional exhaustion, cynicism, and a persistent sense of reduced effectiveness at work
India: Among the fastest-rising concerns in Indian corporate settings; IT, healthcare, and finance sectors most affected
18. Dissociative Disorders
Dissociative disorders involve disruptions in consciousness, memory, identity, or perception, often linked to trauma. They are more prevalent than commonly understood and are frequently misdiagnosed in India.
Key symptom: Episodes of feeling detached from oneself, memory gaps, or experiencing identity confusion
India: Prevalence underestimated in India; cultural idioms of distress sometimes mask dissociative presentations
19. Somatic Symptom Disorders
Somatic disorders involve physical symptoms (pain, fatigue, breathlessness) for which no adequate medical explanation is found, but which are caused or maintained by psychological factors.
Key symptom: Persistent physical complaints without identifiable medical cause, accompanied by significant health anxiety
India: Extremely common in Indian primary care settings; estimated 20 to 30 percent of GP consultations may involve somatic presentations
20. Seasonal Affective Disorder (SAD)
SAD is a subtype of depression that follows a seasonal pattern, typically worsening in winter months. In India, it is less studied than in Western contexts but is clinically recognised.
Key symptom: Recurrent depression with seasonal onset, often with increased sleep, appetite, and low energy
India: Underrecognised in India; may be more prevalent in northern regions with significant seasonal variation
📊 Key Fact
- Depression and anxiety disorders together account for 32 percent of India's mental health market burden (IMARC Group, 2026-2034)
- The two most commonly searched mental health topics in India are depression (symptoms and treatment) and anxiety disorder — reflecting where need and awareness are highest.
Common Signs and Symptoms of Mental Health Problems
One of the most significant barriers to mental health care in India is the failure to recognise symptoms early. Mental health problems do not always announce themselves dramatically. They often begin quietly, through shifts in mood, behaviour, and cognition that are easy to attribute to stress, tiredness, or personality traits. Understanding the early warning signs of mental health problems can meaningfully reduce the delay between onset and treatment-seeking.
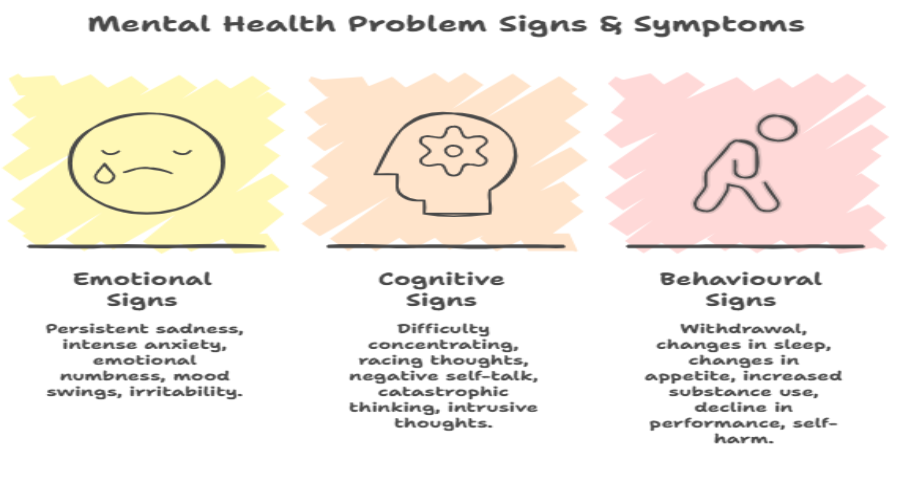
Emotional Signs
- Persistent sadness or low mood lasting more than two weeks
- Intense, prolonged anxiety or a sense of dread that does not correspond to a specific threat
- Emotional numbness or a feeling of emptiness
- Mood swings that are disproportionate or difficult to manage
- Irritability, anger, or frustration that feels excessive or out of character
Cognitive Signs
- Persistent difficulty concentrating, remembering, or making decisions
- Racing or circular thoughts that cannot be quieted
- Negative self-talk or an internal narrative of worthlessness, failure, or hopelessness
- Catastrophic thinking: consistently imagining worst-case outcomes
- Intrusive, unwanted thoughts that cause distress (a potential sign of OCD or PTSD)
Behavioural Signs
- Withdrawal from relationships, social situations, or activities previously enjoyed
- Changes in sleep: significant insomnia or sleeping far more than usual
- Changes in appetite or eating patterns
- Increased use of alcohol, tobacco, or other substances as a coping mechanism
- Decline in work or academic performance not explained by external circumstance.
- Self-harm or thoughts of suicide (seek immediate support: call Tele MANAS at 14416)
When Normal Stress Becomes a Mental Health Problem
Not every difficult period is a clinical mental health condition. Stress, sadness, and anxiety are normal parts of life. The clinical threshold is reached when symptoms persist significantly beyond the trigger event, begin to impair daily functioning (at work, in relationships, in self-care), and do not improve with ordinary coping strategies.

Mental Health Symptoms in Women
Women in India experience higher rates of depression and anxiety than men. NIMHANS data (2019) shows that depression affects 20 percent of Indian women, compared to 10 percent of Indian men. This disparity reflects not just biological factors but the specific stressors Indian women face: domestic violence, gender-based inequality, the pressure of caregiving without support, post-partum depression (affecting 22 percent of Indian mothers), and the cultural expectation to prioritise family well-being over personal distress.
Women in India are also more likely to present with somatic symptoms such as unexplained headaches, fatigue, and digestive complaints when experiencing psychological distress, which can delay a mental health diagnosis if GPs are not trained to look beyond physical presentations.
Mental Health Symptoms in Men
Indian men are significantly less likely to seek mental health support than women, despite high rates of substance use disorders, anger-related presentations, and a notably higher suicide rate. Cultural constructions of masculinity in India, captured in phrases like mard ko dard nahi hota, actively suppress emotional expression and help-seeking in men. Male mental health problems frequently present through externalising behaviours, including irritability, aggression, overwork, and substance use, rather than the internalising symptoms more commonly associated with depression and anxiety in clinical literature.
Male loneliness is a particularly significant and underaddressed contributor to mental health deterioration in India. After marriage, many Indian men's social worlds narrow considerably, leaving them without close confidants. For many men, there is also a disconnect between how they function outwardly and how they feel internally. They may continue to fulfill responsibilities, go to work, and appear “fine” while struggling emotionally in silence. Because vulnerability is often discouraged, many men learn to minimise or ignore their own distress until it reaches a point of significant emotional exhaustion. This contributes to worsening mental health outcomes and is closely linked to India’s high male suicide burden.
⚠️ 70 to 92 percent of people with mental disorders in India do not seek treatment
- The primary barriers are: stigma and shame, lack of mental health literacy, geographic inaccessibility of services, cost of private care, and a cultural preference for spiritual or traditional healing over psychiatric treatment.
- Understanding the warning signs is the first step. Acting on them is the essential second
What Causes Mental Health Problems? Risk Factors in the Indian Context
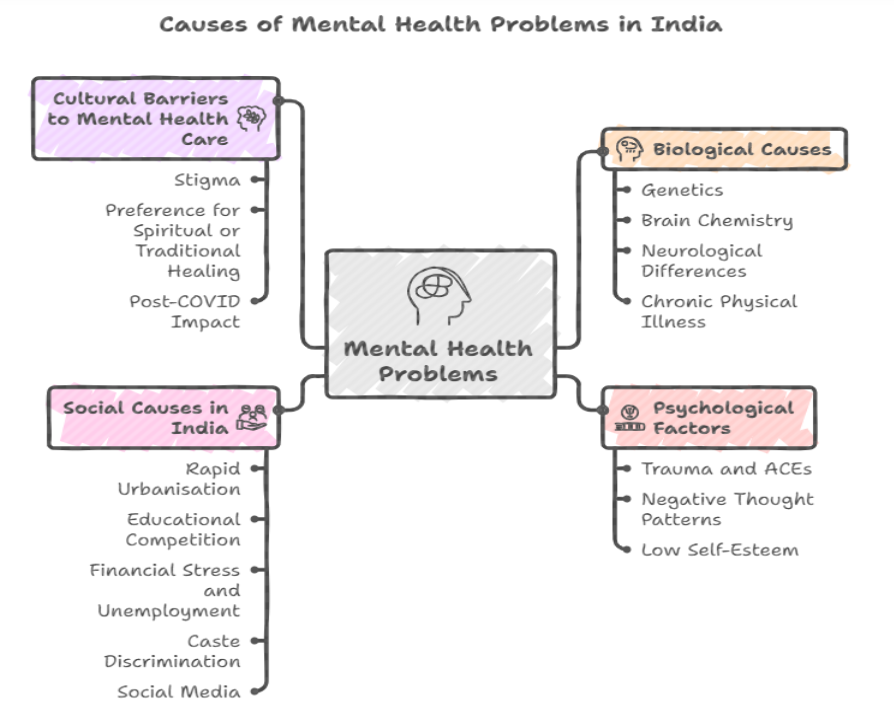
Mental health problems do not have a single cause. They develop through the interaction of biological vulnerability, psychological patterns, and environmental and social factors. In India, several of these factors carry a distinctive weight that is not captured by Western epidemiological frameworks.
Biological Causes
- Genetics: Family history is one of the strongest predictors of mental health conditions. Schizophrenia shows approximately 80 percent heritability; bipolar disorder approximately 70 percent; depression approximately 40 percent. Having a parent or sibling with a mental health condition increases personal risk significantly.
- Brain chemistry: Dysregulation in neurotransmitter systems (serotonin, dopamine, norepinephrine, glutamate) is associated with specific conditions. Selective Serotonin Reuptake Inhibitors (SSRIs) act on serotonin pathways; antipsychotics act primarily on dopamine.
- Neurological differences: Structural and functional brain differences have been identified in conditions including OCD, PTSD, schizophrenia, and ADHD.
- Chronic physical illness: Conditions including diabetes, hypothyroidism, cardiovascular disease, and chronic pain are strongly associated with increased rates of depression and anxiety.
Psychological Factors
- Trauma and adverse childhood experiences (ACEs): Physical, emotional, or sexual abuse, neglect, domestic violence, and early loss are among the strongest predictors of adult mental health conditions.
- Negative thought patterns: Perfectionism, catastrophic thinking, and chronic negative self-evaluation increase vulnerability to anxiety and depression.
- Low self-esteem: Reinforced in India by family comments about weight, academic performance, skin colour, and social comparison.
Social Causes in India
- Rapid urbanisation: Urban prevalence of mental disorders in India (13.5 percent, NIMHANS NMHS 2016) is almost double the rural prevalence (6.9 percent). The severing of community and family networks through migration is a primary driver.
- Educational competition: India's high-stakes examination system creates conditions of sustained psychological pressure from childhood. People between the ages of 18-30 and 30-45 collectively accounted for almost two-thirds (66%) of suicides in the country. (NCRB 2023).
- Financial stress and unemployment: Farmer distress, urban unemployment, and economic precarity are significant mental health risk factors with limited structured support.
- Caste discrimination: The psychological toll of caste-based discrimination is documented but underrepresented in mental health research and clinical practice in India.
- Social media: Comparison culture, cyberbullying, and algorithm-driven anxiety content are rising mental health risk factors, particularly for Indian youth under 25.
Cultural Barriers to Mental Health Care
- Stigma: The fear of being labelled pagal (mad) or damaging family izzat (honour) delays treatment-seeking by an average of 5 to 10 years in India.
- Preference for spiritual or traditional healing: Many Indians first seek help from religious leaders, faith healers, or Ayurvedic practitioners before (or instead of) mental health professionals. While these resources have value, relying on them alone may delay access to evidence-based care when symptoms are severe.
- Post-COVID impact: The WHO estimates that global rates of anxiety and depression rose 25 percent during the pandemic. India saw significant mental health deterioration, with lockdown-era social disconnection creating patterns that, for many, have not fully resolved.
💡 For Indian Workplaces
- The mental health risk factors most prevalent in Indian corporate settings include chronic overwork, lack of psychological safety, financial anxiety, and the absence of social support following relocation.
- The IT sector, with its always-on culture, high attrition, and imposter syndrome prevalence, shows particularly elevated mental health risk.
- EAP (Employee Assistance Programme) counselling is the most accessible first-line intervention for working professionals. Providers such as 1to1help offer confidential, clinician-led support accessible from day one.
How to Improve Mental Health: Practical Tips for Everyday Well-Being
Good mental health is not the default state that exists in the absence of illness. It is something that can be actively cultivated. The following evidence-based steps are adapted for Indian contexts and lifestyles.
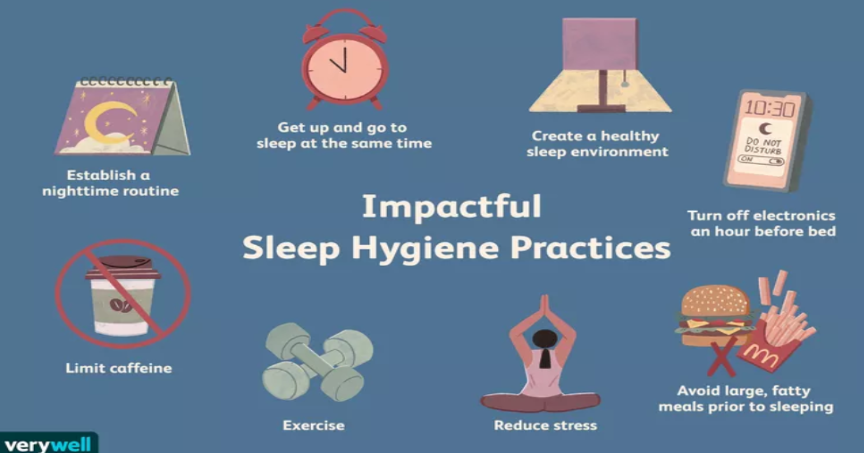
- Physical activity: Thirty minutes of moderate physical activity per day (walking, yoga, swimming, or any sustained movement) reduces symptoms of depression and anxiety by 30 to 40 percent. This is not a supplementary recommendation; it is a primary mental health intervention. Yoga and pranayama, specifically, have demonstrated evidence for reducing cortisol and supporting parasympathetic nervous system activation.
- Sleep hygiene: Seven to nine hours of sleep per night is the clinical recommendation for adults. Irregular sleep is strongly correlated with depression and anxiety in Indian adults. Consistent sleep and wake times, limiting screens before bed, and keeping the bedroom cool and dark are accessible, evidence-based starting points.
- Nutrition: A diet rich in omega-3 fatty acids, B vitamins, and magnesium supports neurological function and is associated with reduced depression risk. Sapien Labs' 2025 global MHQ report found a significant negative correlation between ultra-processed food consumption and mental health scores. Traditional Indian diets, rich in legumes, vegetables, and fermented foods, are broadly supportive of mental wellbeing when not replaced by ultra-processed alternatives.
Recommended Reading:
- 15 Nutrients That Are A Blessing To Your Immune System
- DASH Diet: Complete Guide, Food List, Meal Plan & Benefits for Blood Pressure
- Social connection: Even a single trusted confidant, one person with whom genuine emotional communication is possible, significantly reduces suicide risk and buffers against depression. In an era of widening urban loneliness, actively maintaining and investing in genuine relationships is a mental health priority. See our full guide for practical tips to overcome loneliness.
- Mindfulness and meditation: Mindfulness-Based Stress Reduction (MBSR) and Mindfulness-Based Cognitive Therapy (MBCT) have robust evidence bases for reducing anxiety, preventing depressive relapse, and improving psychological flexibility. In the Indian context, yoga, pranayama, and meditation traditions offer culturally embedded entry points to these practices.

- Digital detox: Limiting social media use to under two hours per day is associated with reduced anxiety among Indian youth. Passive scrolling (consuming others' content without interaction) is consistently more harmful than active use (communicating, organising real-world connection). A deliberate limit on passive consumption is a meaningful mental health intervention.
- Journaling: Writing about emotional experiences, not as performance but as private processing, reduces rumination and supports emotional clarity. In a cultural context where emotional expression is often suppressed, journaling offers a private, low-barrier outlet.
- Seek professional help early: One of the most impactful things a person with persistent mental health symptoms can do is seek professional help before symptoms become severe. Online therapy in India now ranges from Rs 500 to Rs 2,000 per session across providers. There are also free and confidential options available. Government-supported services like Tele MANAS offer 24/7 telephonic support across India. Many workplaces also provide Employee Assistance Programmes (EAPs), which give employees access to free, confidential counselling sessions. The cost of untreated depression, in lost productivity, physical health consequences, and quality of life, far exceeds the cost of early intervention.
Mental Health Tips for Students and Working Professionals in India
Students: Set structured study-break schedules (50 minutes of study, 10 minutes of genuine rest). Speak to your college counsellor; most universities now have student wellness centres. Avoid comparison with peers; academic performance is one dimension of a much broader human life.
Working professionals: Learn to recognise the three stages of burnout (exhaustion, cynicism, reduced efficacy) before they compound. Use EAP services where available; they are confidential and employer-funded. Set boundaries on after-hours messaging.
Parents: Model healthy emotional expression; children learn from watching adults, not lectures. Reduce academic pressure; watch for early warning signs in children, such as school refusal, changes in sleep, or withdrawal.
Elderly: Encourage community participation and social engagement. Monitor for depression presenting as physical complaints, which is particularly common in older Indian adults who may not have a mental health vocabulary for their distress.
✅ Key Principle
- Mental health improvement does not require dramatic change. Small, consistent actions taken across multiple domains (movement, sleep, connection, nutrition) compound over time to produce meaningful shifts in wellbeing.
- Professional help is most effective when sought early. Waiting until a crisis is the most expensive form of mental health care.
Mental Health Treatment Options Available in India
The range of effective mental health treatments available in India has grown significantly over the past decade. The challenge is not that treatments do not exist, but that awareness of them and access to them remain inadequate. The following overview covers all major modalities.
Psychotherapy
Psychotherapy is the use of structured psychological techniques to address mental health conditions. The most evidence-based approaches available in India include:
- Cognitive Behavioural Therapy (CBT): The most researched psychological treatment in the world. CBT addresses the relationship between thoughts, feelings, and behaviours, and is effective for depression, anxiety, OCD, PTSD, eating disorders, and more.
- Exposure and Response Prevention (ERP): The gold-standard treatment for OCD. Involves gradual, structured exposure to feared stimuli while refraining from compulsive responses.
- Dialectical Behaviour Therapy (DBT): Particularly effective for borderline personality disorder, self-harm, and emotional dysregulation. Combines CBT with acceptance and mindfulness strategies.
- EMDR (Eye Movement Desensitisation and Reprocessing): Evidence-based treatment for PTSD and trauma-related conditions. Available from trained therapists in Indian metro cities.
- Interpersonal Therapy (IPT): Particularly effective for depression and binge eating disorder. Focuses on interpersonal stressors and communication patterns.
- Family-Based Treatment (FBT): Particularly relevant for adolescent eating disorders in India's family-centric culture. Parents take an active role in the recovery process.
Medication
Psychiatric medication is prescribed by registered psychiatrists (MBBS + MD/DNB Psychiatry). It is not a standalone treatment for most conditions, but it is highly effective when combined with therapy for moderate-to-severe presentations.
- SSRIs (Selective Serotonin Reuptake Inhibitors): First-line pharmacological treatment for depression, anxiety, OCD, and PTSD. Generic versions are widely available in India at low cost.
- Mood stabilisers: Used in bipolar disorder management. Require regular blood monitoring.
- Antipsychotics: Used in schizophrenia, bipolar disorder with psychosis, and treatment-resistant depression.
Online Therapy in India
Online therapy has significantly improved access to mental health support in India, particularly for those in non-metro areas, individuals with limited mobility, and those who prefer the privacy of digital consultations.
Today, a wide range of platforms offer therapy through video calls, phone sessions, or chat-based support. In addition to individual users, many organisations provide access to counselling through structured workplace programs such as Employee Assistance Programmes (EAPs), which offer confidential, clinician-led support.
Costs typically range from Rs 500 to Rs 2,000 per session, making therapy more accessible than ever before. At the same time, free telephonic services such as Tele-MANAS provide immediate support for those who may not be ready or able to seek paid care.
Government Mental Health Programmes in India
Ayurveda, Yoga, and Integrative Mental Health
India's AYUSH system offers a complementary framework for mental wellness. Mindfulness-based stress reduction (MBSR) has a strong evidence base for reducing anxiety and preventing depressive relapse. Yoga and pranayama are increasingly integrated into formal mental health treatment protocols in India. These approaches are most effective as supplements to, rather than replacements for, evidence-based clinical treatment for diagnosed conditions.
Who to See: Types of Mental Health Professionals in India
India has a significant shortage of mental health professionals. With 0.75 psychiatrists per 100,000 people (against a WHO recommendation of 3), navigating who to see and when is a practical challenge. The following table clarifies the key distinctions.

When to see a counsellor vs psychologist vs psychiatrist: For mild distress, adjustment difficulties, and life transitions, a counsellor or psychologist is the right starting point. For conditions that appear moderate to severe, involve psychotic symptoms, require medication, or have not improved with therapy alone, a psychiatrist is essential. Many people benefit from working with both simultaneously. Look for RCI registration (clinical psychologists) or NMC/MCI registration (psychiatrists) as quality benchmarks. See our complete psychologist vs psychiatrist guide for full details.
Mental Health Across Different Groups in India
Youth Mental Health in India
India has one of the world's youngest populations, and its youth are experiencing a mental health crisis that is growing faster than the infrastructure to address it. They are navigating multiple layers of pressure, from high-stakes academic expectations to constant social comparison and identity-related challenges, often with limited space for rest or emotional processing.
The primary stressors include board examination pressure (Class 10 and 12), preparation for competitive entrance examinations (JEE, NEET, UPSC), social media comparison culture, cyberbullying, and identity-related pressures. At the same time, most Indian schools do not have adequately trained counsellors, and mental health is not formally embedded in the school curriculum, leaving many adolescents to cope without structured support during a critical stage of development.
Workplace Mental Health in India
Poor mental health is one of the most significant drivers of productivity loss, absenteeism, and attrition in Indian organisations. India's IT sector, with its always-on culture, high performance expectations, and significant relocation demands, shows elevated rates of burnout and anxiety. The startup culture compounds this with financial precarity, long hours, and the absence of structured psychological support.
The three stages of burnout (exhaustion, cynicism, and reduced professional efficacy) are often visible long before they are named. Employers have both a moral and a business case for structural responses: EAPs, flexible working, destigmatisation campaigns, and leadership that models help-seeking. The Global Workplace Mental Health Standard (ISO 45003) provides a framework for organisations ready to formalise their approach. See our workplace mental health guide for a comprehensive overview.
Women's Mental Health in India
Women in India often carry an invisible mental load that extends beyond visible responsibilities. Alongside work or household roles, they are frequently expected to manage emotional labour, maintain relationships, and adapt to shifting expectations across different life stages.
Experiences such as domestic conflict, limited autonomy, caregiving without support, and pressure to meet idealised roles can contribute to chronic stress, emotional exhaustion, and untreated mental health concerns. These struggles are often normalised or minimised, which makes it less likely for women to seek help or even recognise their own distress, especially during vulnerable phases such as early motherhood or major life transitions.
Breaking the Stigma: Mental Health Awareness in India
In India, the biggest challenge is often not recognising distress, but feeling unable to act on it. Many people learn early on to manage emotional struggles privately, to avoid worrying their families, or to prevent being judged in social and professional spaces. Mental health concerns are frequently reframed as personal weakness, something to “control,” or something that will pass with time. As a result, individuals continue to function outwardly while their internal distress builds, often reaching a point where intervention becomes more complex, and recovery takes longer.
India's Mental Healthcare Act 2017 was a landmark legal step: it decriminalised suicide, mandated that mental healthcare be accessible and affordable as a right, and prohibited discrimination on the grounds of mental illness. But legal frameworks take decades to change cultural norms. The actual work of destigmatisation happens in families, workplaces, schools, and media.
“When I spoke about my depression, people thought I was weak. I want people to know that it takes strength to ask for help.”
— Deepika Padukone, founder of the Live Love Laugh Foundation
Public figures speaking openly about mental health have a demonstrable effect on public perception. Deepika Padukone's 2015 public disclosure of her depression, and the subsequent founding of the Live Love Laugh Foundation, is credited with a measurable increase in mental health conversations and help-seeking in India. The data consistently shows that contact-based education (hearing from people with lived experience) is more effective at reducing stigma than information campaigns alone.
What individuals can do: Use accurate language (avoid 'crazy', pagal, 'mental'). Support help-seeking without judgement. Educate yourself about specific conditions rather than operating from generalised fear. Normalise conversations about emotional health in your family and workplace.
World Mental Health Day (10 October): India marks World Mental Health Day with growing participation from government, NGOs, and corporate India. The Live Love Laugh Foundation, iCall, and NIMHANS all run annual awareness campaigns. Using these moments to open conversations in your own network has genuine impact.
Mental Health Resources, Helplines and Government Programmes in India
Access to mental health support in India is more varied than most people realise. The following is a structured overview of available resources, from government-funded free services to NGOs and digital platforms.
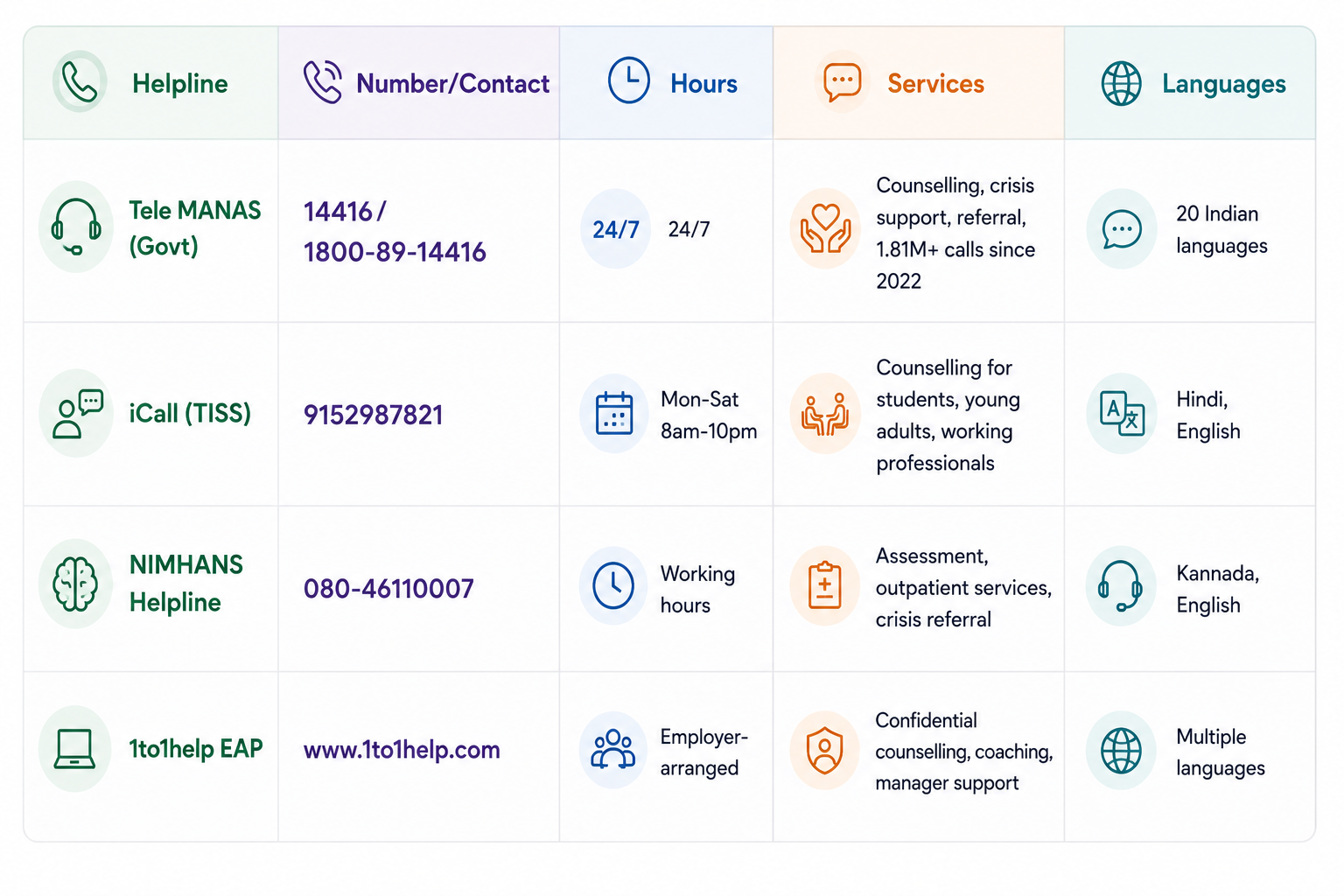
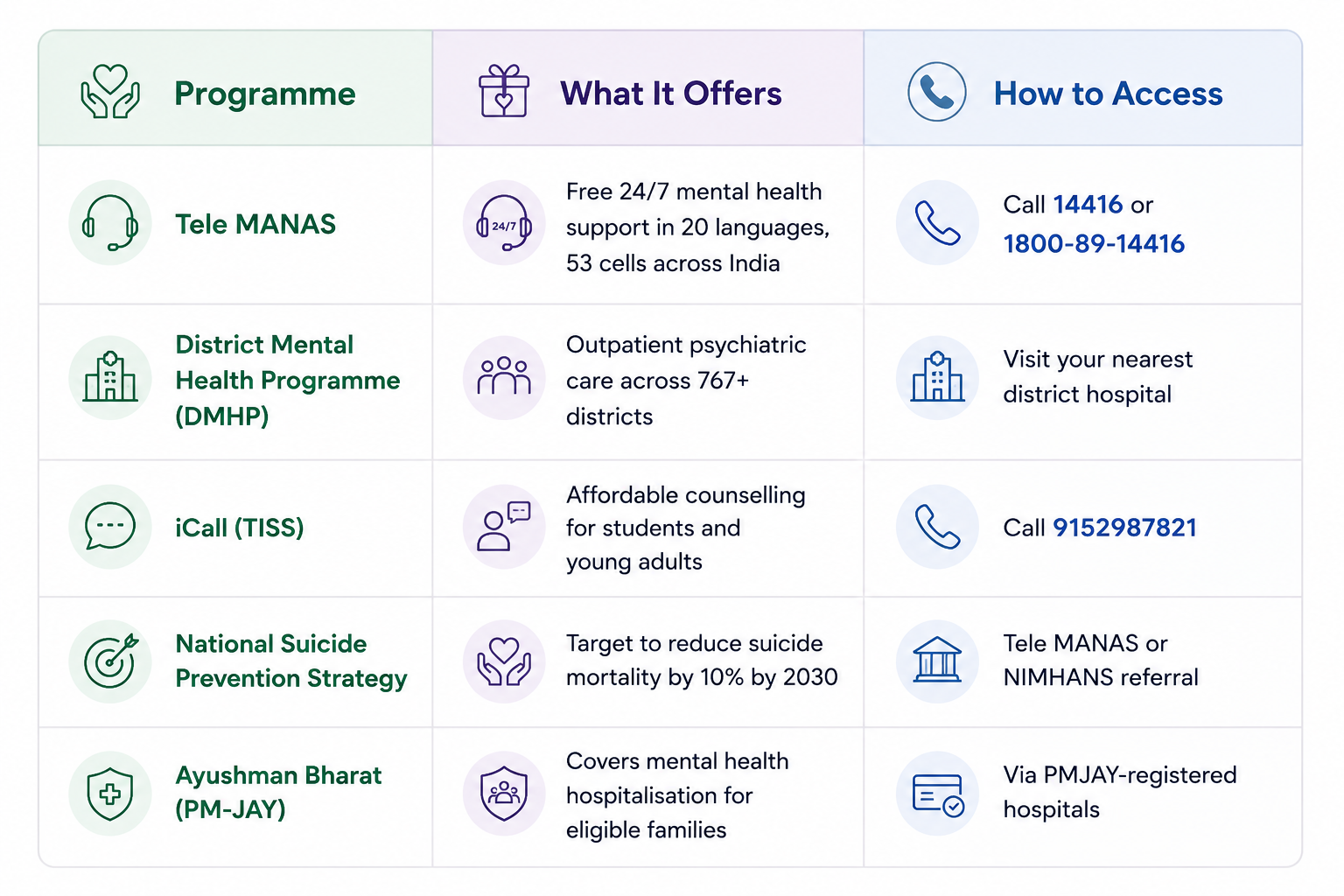
The Tele MANAS national programme has handled over 1.81 million calls since its launch in 2022, making it the largest single mental health access point in Indian history. It is free, available around the clock, and operates across 20 Indian languages. For those in crisis, it should always be the first call.
The National Suicide Prevention Strategy (NSPS) 2022 sets a target of reducing India's suicide mortality rate by 10 percent by 2030. The National Mental Health Programme (NMHP) and District Mental Health Programme now cover 767 districts, bringing primary mental health care closer to communities historically excluded from services.
Explore Our Complete Mental Health Sub-Topic Library
Every condition, topic, and life stage covered in this guide has a dedicated full-length resource in our mental health library. Each guide follows clinical evidence, is written for Indian readers, and is reviewed by mental health professionals.
A Final Word
Arjun, the project manager from our opening, eventually used his company's EAP to speak to a counsellor. Three sessions in, he was able to name what he was experiencing as anxiety, not weakness, not failure, and not something he needed to manage alone. He began working with a clinical psychologist. He also started running three mornings a week, not because running is a cure, but because it helped.
Mental health is not a destination. It is a continuous process of understanding, tending to, and occasionally repairing the most fundamental instrument we have: our own minds. In India, where that process has been made harder than it should be by stigma, access gaps, and cultural silence, naming it, learning about it, and seeking help for it are all acts of genuine courage.
If something in this guide has resonated with you, start with one step. Call Tele MANAS on 14416 or reach out to your EAP helpline. Look up a local psychologist. Share this page with someone who needs it. The treatment gap in India does not close because of policy documents alone. It closes because individuals decide that their mental health is worth the same care and attention as their physical health.
Medical Disclaimer: This content is for informational purposes only and does not constitute medical advice. If you are in crisis, please call Tele MANAS at 14416 immediately or reach out to EAP counselling at your workplace.
FAQs
Q1. What is mental health, and why is it important?
Mental health refers to a person's emotional, psychological, and social well-being. It shapes how we think, feel, and behave every day, influencing our decisions, relationships, stress responses, and overall quality of life. According to the World Health Organization, good mental health is not simply the absence of illness; it is a positive state of well-being that allows individuals to realise their potential, cope with life's stresses, work productively, and contribute to their community. In India, where an estimated 150 million people need care but most do not access it, prioritising mental health leads to better physical health, stronger relationships, higher productivity, and reduced risk of chronic disease.
Q2. How do I know if I have a mental health problem?
Common warning signs include persistent sadness or hopelessness lasting more than two weeks, excessive worry or fear that interferes with daily life, dramatic mood swings, withdrawal from friends and activities you once enjoyed, changes in sleep or appetite, difficulty concentrating, and thoughts of self-harm or suicide. In the Indian context, also watch for physical complaints without a clear medical cause, increased irritability, or a significant drop in academic or work performance. If these signs persist and interfere with daily functioning, speak with a qualified mental health professional. Experiencing these symptoms does not mean weakness. It means you are dealing with a health condition that responds to treatment.
Q3. Is mental health treatment free in India?
Yes there are options available free at cost. Tele MANAS (14416) offers free, round-the-clock counselling in 20 Indian languages. iCall by TISS (9152987821) provides free or affordable counselling for students and young adults. District Mental Health Programme (DMHP) centres across 767 districts offer outpatient psychiatric care at no or very low cost. NIMHANS in Bengaluru provides subsidised specialist services. The Ayushman Bharat PM-JAY scheme covers mental health hospitalisation for eligible families. NGOs also offer subsidised services. Online therapy ranges from Rs 500 to Rs 2,000 per session on most platforms.
Q4. How can I help someone with a mental illness in India?
Supporting someone with a mental illness begins with listening without judgement. Avoid dismissive phrases like 'just be positive' or 'it will pass.' Educate yourself about their specific condition. Gently encourage professional help and offer to accompany them to their first appointment. Be patient: recovery takes time and involves setbacks. Reduce stigma within your family by speaking openly about mental health. In a crisis, particularly if there is any mention of suicide or self-harm, take it seriously and call Tele MANAS at 14416 or reach out to your EAP counsellor (provided by workplace) immediately.
Q5. What is the difference between a psychologist and a psychiatrist in India?
A psychiatrist is a medical doctor with MBBS and MD or DNB in Psychiatry, qualified to diagnose conditions and prescribe medication. A psychologist holds a Masters or Doctoral degree in Psychology, is trained in assessment and therapy, but cannot prescribe medication in India. For mild to moderate conditions, a psychologist or counsellor is often the right starting point. For severe conditions including schizophrenia, bipolar disorder, or treatment-resistant depression, a psychiatrist is essential. Many people benefit from working with both.
Q6. Can mental health problems be cured completely?
Many mental health conditions are highly treatable, and many people achieve full recovery with appropriate support. Conditions like mild to moderate depression and anxiety respond very well to a combination of therapy and lifestyle changes. Others, such as bipolar disorder or schizophrenia, are managed as long-term conditions, much like diabetes or hypertension, where the goal is effective management rather than a single cure. Recovery is not always linear. Early intervention significantly improves outcomes. With the right treatment, most people with mental health disorders can lead fulfilling, productive lives. The key is to seek professional help early, not after a crisis.
Q7. What are the early signs of mental illness in teenagers in India?
Early warning signs in Indian teenagers include a sudden drop in academic performance, withdrawal from family and friends, loss of interest in hobbies, excessive use of social media or video games, significant changes in sleep or eating patterns, and frequent physical complaints without a clear medical cause. More serious signs include persistent sadness, irritability, talk of hopelessness, and any mention of self-harm or suicide. India's 15 to 24 age group accounts for over 35 percent of suicide deaths (NCRB 2023). If you notice these signs, approach the young person gently without judgement, and consult a school counsellor, child psychologist, or call Tele MANAS at 14416 for guidance.
References
- Advanced Psychiatry Associates. (n.d.). Comprehensive guide to understanding and treating ADHD. https://advancedpsychiatryassociates.com/resources/blog/comprehensive-guide-to-understanding-and-treating-adhd
- American Academy of Family Physicians. (2016). Dissociative disorders: Recognition and treatment. https://www.aafp.org/pubs/afp/issues/2016/0101/p49.html
- American Psychiatric Association. (n.d.). Psychotherapy. https://www.psychiatry.org/patients-families/psychotherapy
- Asana. (n.d.). Impostor syndrome: What it is and how to overcome it. https://asana.com/resources/impostor-syndrome
- Association for Talent Development. (2022). Mental health at work standards. International Organization for Standardization. https://www.iso.org/contents/news/2022/04/mental-health-at-work.html
- Brown University School of Professional Studies. (2023). MBSR vs MBCT: Understanding the differences. https://professional.brown.edu/news/2023-11-28/mbsr-vs-mbct
- Centre for Mental Health Law & Policy. (2024). Takeaways from the NCRB data on suicide for 2023. https://cmhlp.org/imho/blog/takeaways-from-the-ncrb-data-on-suicide-for-2023-what-has-changed/
- Child Mind Institute. (n.d.). Family-based treatment for eating disorders. https://childmind.org/article/family-based-treatment-for-eating-disorders/
- Child Mind Institute. (n.d.). Parents’ guide to autism. https://childmind.org/guide/parents-guide-to-autism/
- Cleveland Clinic. (n.d.). Antipsychotic medications. https://my.clevelandclinic.org/health/treatments/24692-antipsychotic-medications
- Cleveland Clinic. (n.d.). Cognitive behavioral therapy (CBT). https://my.clevelandclinic.org/health/treatments/21208-cognitive-behavioral-therapy-cbt
- Cleveland Clinic. (n.d.). Dialectical behavior therapy (DBT). https://my.clevelandclinic.org/health/treatments/22838-dialectical-behavior-therapy-dbt
- Cleveland Clinic. (n.d.). Diabetes. https://my.clevelandclinic.org/health/diseases/7104-diabetes
- Cleveland Clinic. (n.d.). Drug addiction (substance use disorder). https://my.clevelandclinic.org/health/diseases/16652-drug-addiction-substance-use-disorder-sud
- Cleveland Clinic. (n.d.). EMDR therapy. https://my.clevelandclinic.org/health/treatments/22641-emdr-therapy
- Cleveland Clinic. (n.d.). Hypothyroidism. https://my.clevelandclinic.org/health/diseases/12120-hypothyroidism
- Cleveland Clinic. (n.d.). Interpersonal psychotherapy (IPT). https://my.clevelandclinic.org/health/treatments/interpersonal-psychotherapy-ipt
- Cleveland Clinic. (n.d.). Mood stabilizers. https://my.clevelandclinic.org/health/articles/mood-stabilizers
- Cleveland Clinic. (n.d.). Neurotransmitters. https://my.clevelandclinic.org/health/articles/22513-neurotransmitters
- Cleveland Clinic. (n.d.). Parasympathetic nervous system (PSNS). https://my.clevelandclinic.org/health/body/23266-parasympathetic-nervous-system-psns
- Cleveland Clinic. (n.d.). Postpartum depression. https://my.clevelandclinic.org/health/diseases/9312-postpartum-depression
- Cleveland Clinic. (n.d.). Cardiovascular disease. https://my.clevelandclinic.org/health/diseases/21493-cardiovascular-disease
- Cleveland Clinic. (n.d.). Chronic pain. https://my.clevelandclinic.org/health/diseases/4798-chronic-pain
- Deconstructing Stigma. (n.d.). Borderline personality disorder guide. https://deconstructingstigma.org/guides/bpd
- Government of India. (2017). Mental Healthcare Act, 2017. https://www.indiacode.nic.in/bitstream/123456789/2249/1/A2017-10.pdf
- HelpGuide. (n.d.). Journaling for mental health and wellness. https://www.helpguide.org/mental-health/wellbeing/journaling-for-mental-health-and-wellness
- HelpGuide. (n.d.). Seasonal affective disorder (SAD). https://www.helpguide.org/mental-health/depression/seasonal-affective-disorder-sad
- IMARC Group. (2025). India mental health market report. https://www.imarcgroup.com/india-mental-health-market
- Indian Journal of Psychiatry. (2023). Bipolar affective disorder in India: A multi-site study. https://journals.lww.com/indianjpsychiatry/fulltext/2023/65120/bipolar_affective_disorder_in_india__a_multi_site.5.aspx
- Indian Pediatrics. (2024). Autism spectrum disorder in Indian children. https://www.indianpediatrics.net/apr2024/321.pdf
- Investopedia. (n.d.). Presenteeism definition. https://www.investopedia.com/terms/p/presenteeism.asp
- International OCD Foundation. (n.d.). Exposure and response prevention (ERP) therapy. https://iocdf.org/about-ocd/treatment/erp/
- MedlinePlus. (n.d.). Mental health. https://medlineplus.gov/mentalhealth.html
- Mind. (n.d.). Causes of mental health problems. https://www.mind.org.uk/information-support/types-of-mental-health-problems/mental-health-problems-introduction/causes/
- MindVoyage. (2025). Latest statistics of anxiety disorders in India. https://mindvoyage.in/latest-statistics-of-anxiety-disorders-in-india/
- Ministry of Health and Family Welfare, Government of India. (n.d.). National Mental Health Programme. https://dghs.mohfw.gov.in/national-mental-health-programme.php
- Ministry of Health and Family Welfare, Government of India. (n.d.). Tele-MANAS. https://telemanas.mohfw.gov.in/home
- National Health Service. (n.d.). Five steps to mental wellbeing. https://www.nhs.uk/mental-health/self-help/guides-tools-and-activities/five-steps-to-mental-wellbeing/
- NDTV. (2023). Alarming rise in suicides by Indian men between 2014 and 2021: Lancet study. https://www.ndtv.com/india-news/alarming-rise-in-suicides-by-indian-men-between-2014-and-2021-lancet-study-4338759
- Press Information Bureau, Government of India. (2024). Mental health initiatives in India. https://www.pib.gov.in/PressReleasePage.aspx?PRID=2188003®=3&lang=2
- Sapien Labs. (2026). Global mind health report 2025. https://sapienlabs.org/wp-content/uploads/2026/02/Global-Mind-Health-in-2025-Report.pdf
- Stanford Medicine. (n.d.). Depression and genetics. https://med.stanford.edu/depressiongenetics/mddandgenes.html
- The Hindu. (2024). Indian youths rank 60 in 84-nation mental health study. https://www.thehindu.com/sci-tech/health/indian-youths-rank-60-in-84-nation-mental-health-study-older-people-perform-better/article70691375.ece
- The Live Love Laugh Foundation. (n.d.). Mental health awareness initiatives. https://www.thelivelovelaughfoundation.org/
- The New Indian Express. (2024). Breaking the silence: Addressing India’s depression crisis. https://www.newindianexpress.com/cities/kochi/2024/Oct/09/breaking-the-silence-addressing-indias-depression-crisis
- Times of India. (2025). India’s sleep crisis: How insomnia is fuelling a billion-rupee industry. https://timesofindia.indiatimes.com/science/indias-sleep-crisis-how-insomnia-is-fuelling-a-billion-rupee-industry/articleshow/130039831.cms
- Verywell Mind. (n.d.). Negative self-talk and how it affects us. https://www.verywellmind.com/negative-self-talk-and-how-it-affects-us-4161304
- Verywell Mind. (n.d.). Signs you may be a perfectionist. https://www.verywellmind.com/signs-you-may-be-a-perfectionist-3145233
- WebMD. (n.d.). What causes schizophrenia? https://www.webmd.com/schizophrenia/what-causes-schizophrenia
- World Health Organization. (2022). COVID-19 pandemic triggers 25% increase in prevalence of anxiety and depression worldwide. https://www.who.int/news/item/02-03-2022-covid-19-pandemic-triggers-25-increase-in-prevalence-of-anxiety-and-depression-worldwide
- World Health Organization. (n.d.). Mental health: Strengthening our response. https://www.who.int/news-room/fact-sheets/detail/mental-health-strengthening-our-response
- World Health Organization India. (n.d.). Mental health in India. https://www.who.int/india/health-topics/mental-health