
.png)

Mental Health Concerns
Phobias: Complete List A–Z, Types, Common Phobias & How to Overcome Fear
.png)
Written by
Aarohi Parakh,
Psychologist and Content Writer

Reviewed by
Sanjana Sivaram,
Psychologist and Clinical Content Head






Introduction

Rohan is a 26-year-old software developer in Bengaluru. He is good at his job, well-liked by his team, and fiercely independent. But every Monday, when his company sends a meeting invite that involves the office lift, he takes the stairs. All fourteen floors of them. He tells colleagues it is for fitness.
What he does not say is that enclosed spaces make him uneasy in a way he cannot quite explain. That stepping into a lift sometimes feels like the air is thinning, like the walls are a little too close. That if he finds himself stuck in a crowded queue near a closed door, it can take several minutes for his breathing to settle again.
Rohan does not think of this as a problem. It is simply something he has learned to work around. He is living with claustrophobia, a specific phobia that millions of people in India manage in silence, often for years, before ever seeking help.
Phobias are one of the most common mental health conditions in the world, and yet they remain among the most misunderstood. They are frequently dismissed as personality quirks, unaddressed childhood fears, or simple oversensitivity. In India, cultural stoicism, stigma, and a lack of mental health literacy mean that most people with phobias never receive a diagnosis, let alone treatment. This is a problem because phobias are also among the most treatable mental health conditions in existence.
This guide covers the definition, types, complete A-Z list, causes, and treatment of phobias, with specific attention to how they present and are understood in the Indian context.
What Are Phobias? Meaning and Definition
A phobia is an intense, irrational, and persistent fear of a specific object, situation, or activity that is disproportionate to the actual danger it poses. The word itself comes from the Greek term “phobos”, meaning fear or dread. Unlike generalised worry or normal apprehension, a phobia triggers a severe and immediate anxiety response, even when the person knows, on a cognitive level, that the threat is minimal or non-existent.
Three elements define a phobia: intense fear, active avoidance, and the recognition of irrationality. The person typically knows their fear is disproportionate to the actual threat, but cannot control their reaction. A phobia becomes clinically significant when the symptoms last for at least 6 months and cause meaningful distress or interfere with daily life, whether that is taking multiple flights of stairs instead of a lift, refusing to visit friends because they have a dog, or missing a flight for an important business trip.
The DSM-5 classifies phobias under Anxiety Disorders and organises specific phobias into five subtypes based on the nature of the feared stimulus. Technically, there are hundreds of named phobias, though most clinicians use the DSM-5's categorical framework rather than individual named diagnoses.
How common are phobias? Specific or simple phobias are among the most common anxiety disorders globally, affecting an estimated 7–9% of people over their lifetime, based on diagnostic data from the American Psychiatric Association and large international epidemiological studies. Indian research, including data from studies indexed in PubMed Central, suggests a prevalence of approximately 4–5%. However, these estimates are based on regional samples, and the true burden is likely higher due to underreporting and limited nationwide data.

Types of Phobias: The 5 Major Categories
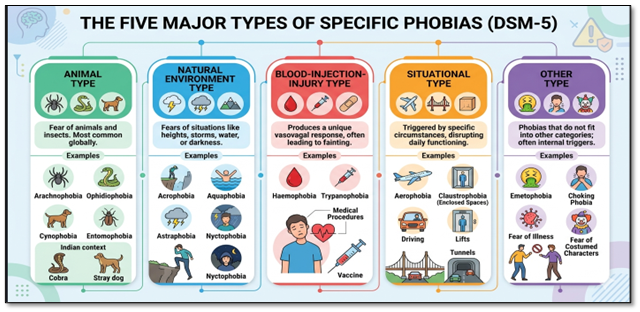
The DSM-5 organises specific phobias into five major categories based on the nature of the feared stimulus. Understanding these categories matters because the treatment approach, the typical age of onset, and the physiological response can differ meaningfully between subtypes. Specific Or Simple Phobias produce intense fear of a particular object or situation that is, in fact, relatively safe.
1. Animal Type
The most common subtype globally and in India. Animal type phobias include arachnophobia (spiders), ophidiophobia (snakes), cynophobia (dogs), and entomophobia (insects). In the Indian context, snake phobias and dog phobias carry particular weight, given real environmental exposure to venomous snakes in semi-urban and rural settings and the prevalence of stray dogs in most Indian cities. The fine clinical distinction is not whether the animal is genuinely dangerous, but whether the fear response is disproportionate and significantly limiting.
Case Example: A 24-year-old woman from Mumbai avoids visiting her relatives in their hometown after a childhood memory of seeing a snake in the backyard. She laughs it off when family members tease her, but even scrolling past a photo of a snake on her phone makes her heart race. She avoids parks, nature trips, and even certain TV shows. The fear is not just about the animal but about the loss of control and the overwhelming panic associated with the stimulus.
2. Natural Environment Type
This subtype includes fears of heights (acrophobia), water (aquaphobia), storms (astraphobia), and darkness (nyctophobia). These phobias often have roots in evolutionary psychology: humans have a pre-wired sensitivity to environments that were genuinely dangerous to our ancestors. In children, nyctophobia is particularly common and is often normalised when it should be taken seriously if it persists beyond early childhood or significantly disrupts sleep and daily functioning.
Case Example: A 10-year-old child refuses to sleep alone at night. What started as a normal fear of darkness has slowly become something more persistent. On nights when the lights go out, especially during power cuts, the child becomes visibly distressed and repeatedly calls out for a parent. Mornings are harder now, with poor sleep affecting school and mood. For the family, it feels like “just a phase,” but it has begun to impact daily functioning.
3. Blood-Injection-Injury Type
This subtype is unique in that it produces a vasovagal response: the heart rate drops rather than rises, frequently causing fainting. It includes fear of blood (haemophobia), needles (trypanophobia), and medical procedures. In India, needle phobia is a significant public health concern because it is one of the leading reasons for vaccine hesitancy and avoidance of necessary medical care. Many people with blood-injection-injury phobia present to GPs with a physical complaint rather than identifying the fear itself.
Case Example: A 19-year-old college student dreads medical visits. During a routine blood test, he faints, and the experience stays with him. Now, even talking about injections makes him feel lightheaded. He delays vaccinations and avoids doctor visits unless absolutely necessary. His family initially assumes it is “weakness,” but clinically, this reflects a vasovagal response associated with needle phobia (trypanophobia), leading to avoidance of essential healthcare.
4. Situational Type
Situational phobias are triggered by specific circumstances rather than objects or animals. This subtype includes flying (aerophobia), driving, enclosed spaces (claustrophobia), lifts, bridges, and tunnels. The workplace relevance here is high: situational phobias are among the most functionally disruptive because they can directly affect commuting, travel for work, and the use of ordinary infrastructure, such as underground metro systems.
Case Example: A 32-year-old corporate employee avoids using the Mumbai Metro, even though it would cut her commute time in half. She prefers longer, more tiring routes just to avoid enclosed spaces. There have been moments when she has stepped out of a lift halfway through because the discomfort felt unbearable. She has quietly turned down travel-related opportunities at work, telling herself it is a choice, even though it often does not feel like one
5. Other Type
This catch-all category includes phobias that do not fit neatly into the four above, such as emetophobia (fear of vomiting), choking phobia, fear of illness, and fear of costumed characters. These phobias can be particularly complex to treat because the feared stimulus is sometimes internal rather than external.
Case Example: A 27-year-old man becomes extremely cautious about food after a severe episode of food poisoning. At first, it seems reasonable. But over time, he begins avoiding eating outside altogether and sticks to a very limited set of “safe” foods. Even a slight feeling of nausea makes him anxious. He often asks others whether the food is safe or repeatedly checks expiry dates. Over time, his fear shifts inward, and he becomes hyper-aware of bodily sensations like nausea, leading to anticipatory anxiety and avoidance behaviors that affect nutrition and social life.
💡Indian Workplace Context
- Situational phobias (claustrophobia, aerophobia) are among the most common reasons Indian employees quietly decline travel assignments or avoid using office lifts.
- EAP (Employee Assistance Programme) counselling, where available, offers a confidential first step for employees who would not otherwise seek help.
Managers who notice consistent avoidance behaviours may be observing an unaddressed phobia, not resistance to work.
In addition to specific phobias, two other anxiety conditions are classified separately in the DSM-5 but are commonly grouped under the phobia umbrella. Social phobia (social anxiety disorder) involves intense fear of social situations where one might be judged, humiliated, or scrutinised.
Agoraphobia involves fear of situations from which escape might be difficult, such as crowded markets, public transport, or being outside the home alone. Both conditions are prevalent in India and are addressed in their respective guides.
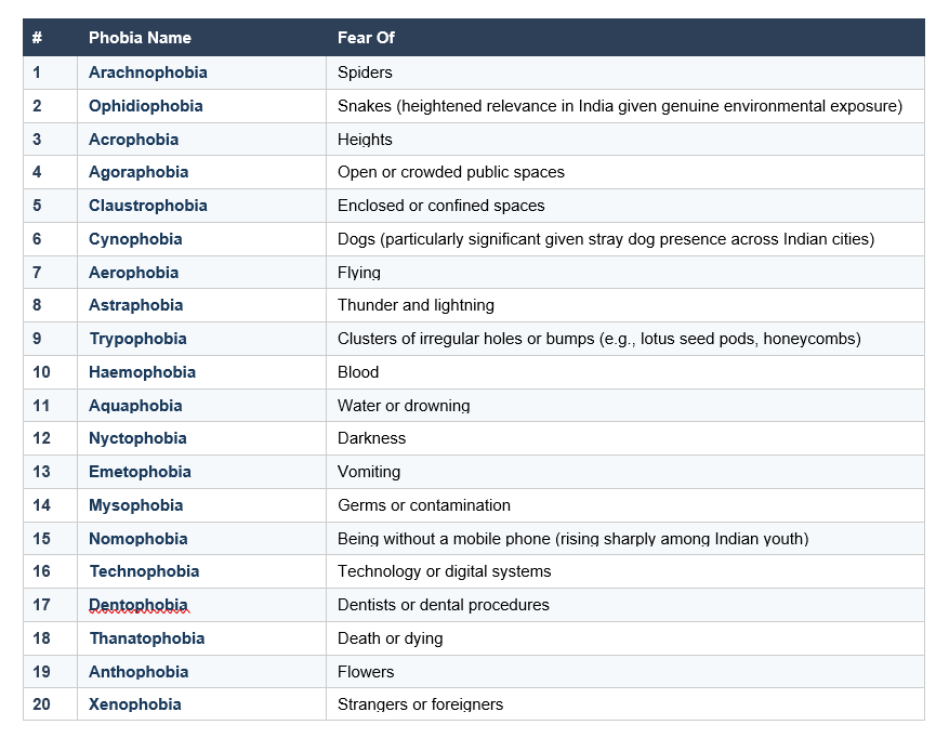
Most Common Phobias in India: A Ranked List
The following list draws on global prevalence data, India-specific search patterns, and clinical presentations common in Indian mental health settings. The ranking reflects both clinical frequency and the particular cultural and environmental factors that shape fear in the Indian context.
A Note on Trypophobia
Trypophobia deserves specific attention because it generates significant search volume and is widely misunderstood. It describes an intense discomfort or fear triggered by irregular clusters of holes, bumps, or circles, such as lotus seed pods, honeycombs, sponges, or certain skin textures. The response is often one of revulsion and physical discomfort rather than classic fear. Research published in Psychological Science suggests that up to 16 percent of people experience it to some degree. Trypophobia is not yet formally classified in the DSM-5, though it is widely discussed in clinical literature. For most people it causes discomfort rather than clinical impairment; for those whose daily life is significantly affected, gradual desensitisation can help.
Culturally Embedded Phobias in India
India has several fear experiences that straddle the boundary between cultural belief and clinical phobia. Fear of the evil eye (drishti or nazar) can reach phobic intensity in some individuals, resulting in compulsive protective rituals and significant anxiety. Fear of ghosts (bhoot phobia) is common among children and in some adults, particularly in rural settings, and is frequently reinforced by family narratives and popular media. These fears are not inherently pathological: the distinction, as always, lies in whether they cause significant distress or meaningful impairment in functioning.
Unusual and Curiosity Phobias
Beyond the most common phobias, hundreds of named fears have been documented, many of which attract curiosity-driven attention online. Some examples include:
- xanthophobia (fear of the colour yellow),
- ergophobia (fear of work),
- arithmophobia (fear of numbers),
- ablutophobia (fear of bathing), and
- the much-cited hippopotomonstrosesquippedaliophobia, the ironic fear of long words.
Nomophobia, the fear of being without a mobile phone, is increasingly prevalent among Indian youth and carries real clinical weight in a country with one of the world's highest smartphone usage rates. Any of these fears, no matter how unusual they seem, can cause genuine distress and are treatable.
List of Phobias A to Z: 100+ Named Phobias
The following list provides a comprehensive reference of named phobias in alphabetical order. It addresses both 'list of phobias a to z' and 'all phobias' as a clinically accurate, scannable resource.
A–F
- Ablutophobia: Fear of bathing or washing
- Acrophobia: Fear of heights
- Aerophobia: Fear of flying
- Agoraphobia: Fear of open or crowded spaces, or situations difficult to escape
- Algophobia: Fear of pain
- Amaxophobia: Fear of riding in a car
- Anthropophobia: Fear of people or human interaction
- Anthophobia: Fear of flowers
- Arachnophobia: Fear of spiders
- Arithmophobia: Fear of numbers
- Astraphobia: Fear of thunder and lightning
- Atychiphobia: Fear of failure
- Autophobia: Fear of being alone or isolated
- Aquaphobia: Fear of water
- Bibliophobia: Fear of books
- Botanophobia: Fear of plants
- Cacophobia: Fear of ugliness
- Catoptrophobia: Fear of mirrors
- Chromophobia: Fear of colours
- Claustrophobia: Fear of confined or enclosed spaces
- Coulrophobia: Fear of clowns or costumed characters
- Cynophobia: Fear of dogs
- Decidophobia: Fear of making decisions
- Dendrophobia: Fear of trees
- Dentophobia: Fear of dentists or dental procedures
- Disposophobia: Fear of getting rid of objects (hoarding-linked)
- Emetophobia: Fear of vomiting
- Entomophobia: Fear of insects
- Ergophobia: Fear of work or workplace environments, often linked to anxiety or burnout
- Frigophobia: Fear of cold temperatures
G–L
- Gamophobia: Fear of marriage or commitment
- Genuphobia: Fear of knees
- Gerascophobia: Fear of growing old
- Glossophobia: Fear of public speaking
- Gynophobia: Fear of women
- Haemophobia: Fear of blood
- Haphephobia: Fear of being touched
- Herpetophobia: Fear of reptiles or amphibians
- Hippopotomonstrosesquippedaliophobia: Fear of long words
- Hydrophobia: Fear of water (in medicine also associated with rabies symptoms)
- Ichthyophobia: Fear of fish
- Latrophobia: Fear of doctors or medical visits
- Katsaridaphobia: Fear of cockroaches (highly relevant in urban India)
- Kenophobia: Fear of empty spaces or voids
- Kleptophobia-adjacent fears: Fear of legal consequences related to stealing
- Koumpounophobia: Fear of buttons
- Latrophobia: Fear of hospitals
- Ligyrophobia: Fear of loud noises
- Lilapsophobia: Fear of tornadoes or hurricanes
- Lockiophobia: Fear of childbirth
M–R
- Megalophobia: Fear of large objects
- Melanophobia: Fear of the colour black
- Microphobia: Fear of small objects or germs
- Mysophobia: Fear of germs or contamination
- Necrophobia: Fear of death or dead things
- Neophobia: Fear of new things or change
- Nomophobia: Fear or anxiety about being without a mobile phone or connectivity
- Nosocomephobia: Fear of hospitals
- Nyctophobia: Fear of darkness
- Obesophobia: Fear of weight gain
- Ochophobia: Fear of vehicles, especially being in traffic or riding in vehicles
- Ophidiophobia: Fear of snakes
- Ornithophobia: Fear of birds
- Papyrophobia: Fear of paper
- Parasitophobia: Fear of parasites
- Pathophobia: Fear of disease or illness
- Phasmophobia: Fear of ghosts
- Pteromerhanophobia: Fear of flying
- Pyrophobia: Fear of fire
- Radiophobia: Fear of radiation
S–Z
- Scopophobia: Fear of being stared at
- Social phobia: Fear of social situations (social anxiety disorder)
- Somniphobia: Fear of sleep
- Spectrophobia: Fear of ghosts or reflections
- Taphophobia: Fear of being buried alive
- Technophobia: Fear of technology
- Thanatophobia: Fear of death
- Trypanophobia: Fear of needles or injections
- Trypophobia: Fear of clusters of irregular holes
- Uranophobia: Fear of heaven, the sky, or the afterlife
- Venustraphobia Fear of attractive women (often linked to social anxiety or self-esteem concerns)
- Verbophobia: Fear of words
- Wiccaphobia: Fear of witches or witchcraft
- Xanthophobia: Fear of the colour yellow
- Xenophobia: Fear of strangers or foreigners
- Xylophobia: Fear of wooden objects or forests
- Zoophobia: Fear of animals in general
Symptoms of Phobias
Phobias are more than everyday fears. They trigger intense emotional, physical, and behavioral reactions when a person is exposed to, or even thinks about, the feared object or situation. While specific phobia and agoraphobia differ in what triggers them, the symptom pattern is often similar.
1. Emotional and Cognitive Symptoms
These affect how you think and feel:
- Intense, overwhelming fear that feels out of proportion to the situation
- Sudden panic or a strong urge to escape
- Feeling like you are in immediate danger, even when you are safe
- Difficulty thinking clearly or concentrating
- Feeling disconnected from yourself (depersonalisation) or your surroundings (derealisation)
2. Physical Symptoms
These are the body’s fear response (often similar to a panic attack):
- Rapid heartbeat or palpitations
- Sweating, chills, or feeling unusually hot
- Shaking or trembling
- Nausea, stomach discomfort, or urge to vomit
- Chest tightness or pain
- Difficulty breathing or feeling smothered
- Dizziness or lightheadedness
- Fainting (especially common in blood-injection-injury phobia)
- Pale skin or “blood draining” sensation
- Tunnel vision or blurred vision
3. Behavioural Symptoms
These show up in how a person adapts their life around the fear:
- Avoiding specific places, objects, or situations at all costs
- Changing routines or lifestyle to prevent exposure to triggers
- Delaying or avoiding important activities (e.g., medical visits, travel, career opportunities)
- Relying heavily on others for a sense of safety
Symptoms in Children
Children may express phobias differently:
- Crying or sudden emotional outbursts
- Tantrums when faced with the feared situation
- Freezing or becoming unusually still
- Clinging tightly to a caregiver or refusing separation
When to Seek Professional Help
Consider seeking professional support if:
- Your fear of a specific object, situation, or activity is significantly limiting your daily life, work, or social activities.
- You are going out of your way to avoid the feared stimulus, including refusing opportunities or altering routines substantially.
- The fear has been present for six months or more and shows no sign of reducing on its own.
- You are experiencing physical symptoms such as panic attacks, fainting, or severe nausea in response to the feared stimulus.
- The avoidance is affecting your professional life, for example refusing travel, avoiding the metro, or declining meetings in specific environments.
- You feel embarrassed or ashamed about the fear and have been managing it in silence.
Phobias are highly treatable, especially with approaches like Cognitive Behavioural Therapy (CBT) and exposure-based techniques.
Where to Get Help in India
- Tele MANAS (Dial 14416)
A free, 24/7 government-supported mental health helpline offering immediate emotional support.
- EAP providers such as 1to1help
Provides confidential counselling through Employee Assistance Programmes (EAPs), including therapy for anxiety and phobias.
- You can also consult a clinical psychologist or psychiatrist for structured treatment and diagnosis.
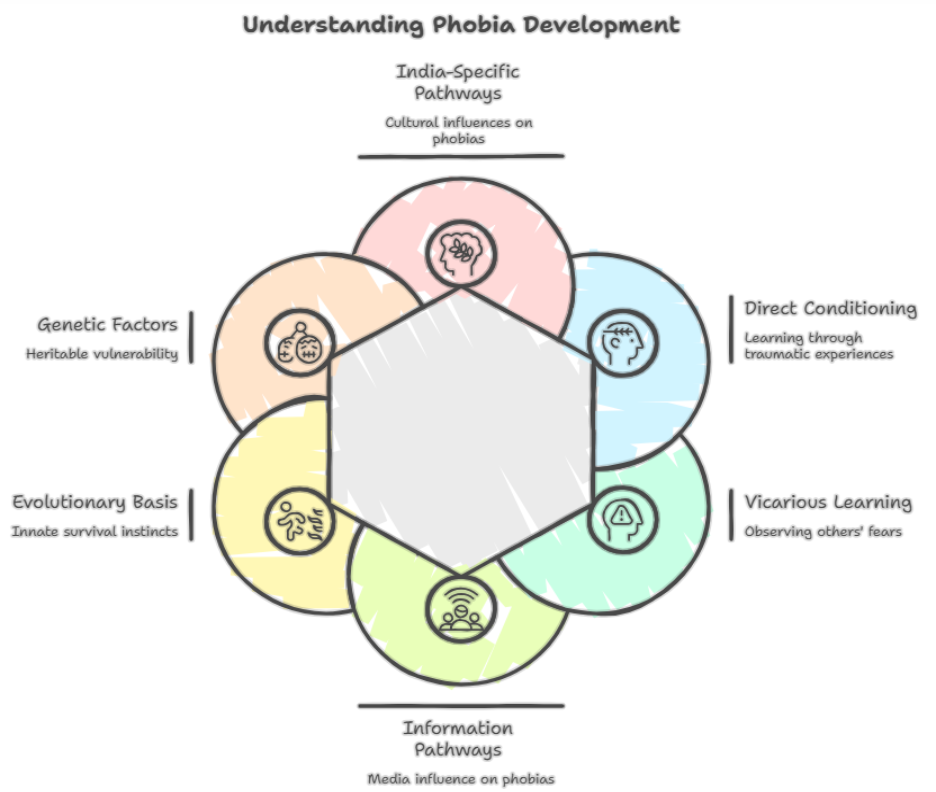
What Causes Phobias? How Do They Develop?
Phobias do not appear from nowhere. They develop through a combination of biological predisposition, learning experiences, and environmental factors. Understanding how a phobia develops is important not only for clinical treatment but for reducing the shame and self-blame that many people with phobias carry.
Direct Conditioning
The most straightforward pathway: a frightening or traumatic experience creates an association between a stimulus and danger. A child bitten by a dog may develop cynophobia. Someone involved in a road accident may develop amaxophobia. The original fear response is rational; the phobia develops when the fear generalises, persists, and becomes disproportionate to actual risk.
Vicarious Learning
Phobias can develop simply by watching others experience fear. A child whose parent screams at the sight of a spider is learning, at a neural level, that spiders are dangerous. This mechanism is particularly relevant in Indian family settings, where children are in close proximity to extended family members and absorb their emotional responses from an early age. The fear does not require a direct encounter with the feared stimulus at all.
Information and Media Pathways
News coverage, horror films, and social media content can all seed or reinforce phobias. The Bollywood horror genre, with its sustained focus on ghosts, dark spaces, and supernatural threats, plays a culturally specific role in shaping and amplifying fear responses in Indian audiences. The rise of short-form video content has accelerated the dissemination of fear-inducing imagery, including trypophobic visuals, to very large audiences.
Evolutionary Basis
Many of the most common phobias reflect fears with genuine evolutionary survival value. The heightened sensitivity to snakes, spiders, heights, and darkness is not irrational in an evolutionary sense: these were real threats for most of human history. Research by Ohman and Mineka demonstrates that humans acquire snake and spider phobias far more easily than phobias of genuinely modern dangers such as cars or electrical outlets, which are objectively more dangerous. This evolutionary preparedness explains why animal phobias are so globally prevalent and why they can be triggered by even stylised or cartoon representations of the feared animal.
Genetic Factors
Phobias have a meaningful heritable component. Twin studies suggest approximately 30 to 40 percent heritability for specific phobias, meaning that genetic factors explain roughly a third of an individual's vulnerability. This does not mean phobias are fixed or untreatable; it means that some individuals have a lower threshold for developing phobic responses when exposed to frightening experiences. The types with higher rates in family members are animal, blood/medical procedure/injury, and situational phobias.
India-Specific Developmental Pathways
In India, several culturally specific pathways shape the development of phobias. Fear of darkness is frequently amplified by childhood ghost narratives embedded in family storytelling and popular culture. Fear of dogs develops in a context where stray dogs are an everyday reality in most Indian cities, making early negative experiences common. Fear associated with the supernatural or the evil eye can develop in contexts where these beliefs are socially reinforced, occasionally escalating to clinical phobia level through repeated ritual anxiety.

How to Overcome Phobias: Treatment That Works
Specific phobias are among the most treatable mental health conditions in existence. The key word is treatable: phobias are not character flaws, and they are not permanent. With the right intervention, most people experience drastic and lasting improvement.
Exposure Therapy: The Gold Standard
Exposure therapy, formally known as systematic desensitisation or graded exposure, is the gold-standard treatment for specific phobias. It works by gradually and systematically exposing the person to the feared stimulus in a safe, controlled setting, allowing the fear response to diminish through a process called habituation. The exposure begins with the least anxiety-provoking scenarios and works upward through a fear hierarchy. The American Psychological Association identifies exposure therapy as the most empirically supported treatment for phobias.
One-Session Treatment
Studies show success rates of up to 80 to 90% for certain specific phobias. Research by Lars-Goran Ost, who developed the one-session treatment model, shows that a single intensive session produces outcomes equivalent to multiple sessions of standard exposure therapy for many specific phobias. This is clinically significant in India, where access to ongoing therapy can be limited by cost, geography, or time constraints.
Cognitive Behavioural Therapy (CBT)
CBT addresses the irrational beliefs and thinking patterns that maintain a phobia. For example, someone with aerophobia may hold the catastrophic belief that any turbulence is a prelude to a crash. CBT helps identify, challenge, and replace these beliefs with more realistic appraisals. CBT is particularly effective for social phobia, which typically requires 12 to 20 sessions due to the complexity of social cognition.
Virtual Reality Exposure Therapy (VRET)
Virtual Reality Exposure Therapy is an increasingly available option in Indian metropolitan centres, particularly for aerophobia, acrophobia, and arachnophobia. VRET allows controlled exposure to feared stimuli in a simulated environment before progressing to real-world exposure. This is particularly valuable for phobias where real-world exposure is difficult to stage in a clinical setting, such as flying.
Self-Help and Gradual Exposure
For mild phobias, structured self-exposure using a personally designed fear hierarchy can be effective. This involves listing feared scenarios from least to most frightening, then working through them progressively over the course of weeks. Self-help approaches work best for milder, situationally bounded phobias and are less effective for phobias with high baseline anxiety, a strong avoidance history, or significant comorbid conditions.
Medication
Medication does not cure phobias but can be useful in specific contexts. Beta-blockers such as propranolol reduce the physical symptoms of anxiety (trembling, rapid heartbeat) and can be helpful for one-off high-anxiety situations such as a flight or a medical procedure. Selective serotonin reuptake inhibitors (SSRIs) are the first-line pharmacological treatment for social phobia and agoraphobia. Short-term benzodiazepines may be prescribed for specific procedural situations, such as needle phobia in a dental or vaccination context, but are not recommended as a standalone treatment because they do not address the underlying fear.
Recovery from a specific phobia is realistic. Most people see a drastic improvement after 1 to 8 sessions of exposure-based therapy. The key is willingness to engage with exposure: sustained avoidance maintains the phobia indefinitely, while even small steps of gradual confrontation begin to reduce it. If you are looking for professional support, online and offline therapy options in India are now accessible, confidential, and clinically effective.
Conclusion: Phobias Are Treatable And You Don’t Have to Live Around Fear
Rohan still works in the same office in Bengaluru. The difference is that he no longer plans his day around avoiding the lift. With structured exposure therapy, what once felt like suffocation now feels manageable. The first few sessions were uncomfortable. They always are. But over time, the panic reduced, the recovery time shortened, and the sense of control returned. Today, he takes the lift, not because the fear has magically disappeared, but because it no longer dictates his behaviour.
That is the shift therapy enables.
Phobias often shrink lives quietly. They do not always look dramatic. They look like taking the stairs every day, avoiding travel, skipping medical appointments, or turning down opportunities. Over time, these adjustments become invisible, even to the person experiencing them.
But phobias are not permanent. They are learned responses, and what is learned can be unlearned.
If you recognise yourself in Rohan’s story, or in any of the patterns described in this guide, support is available. Tele MANAS (Dial 14416) offers free 24/7 mental health support, 1to1help provides confidential counselling for working professionals through EAP, and you can also consult a clinical psychologist or psychiatrist for structured, evidence-based treatment.
The most important step is not eliminating fear completely. It is reducing its control over your choices.
Because the goal is not to never feel fear again.
The goal is to live your life without organising it around fear.

FAQs
Q1. What is a phobia, and how is it different from normal fear?
A phobia is an intense, irrational, and persistent fear of a specific object, situation, or activity that is out of proportion to the actual danger. Unlike normal fear, which is a healthy and adaptive response to genuine threats, a phobia triggers a severe anxiety response even to harmless or low-risk situations. The person typically recognises that their fear is irrational but cannot control the response. A phobia becomes clinically significant when it causes significant distress or leads to avoidance that interferes with daily life. For example, someone with a dog phobia who avoids parks, friends' homes, and outdoor spaces in order to prevent encountering a dog has a clinically significant phobia that warrants treatment.
Q2. What are the most common phobias?
The most common phobias worldwide, and in India, include arachnophobia (spiders), ophidiophobia (snakes), acrophobia (heights), agoraphobia (open or crowded spaces), claustrophobia (enclosed spaces), aerophobia (flying), and cynophobia (dogs). In India, snake and dog phobias are particularly prevalent due to direct environmental exposure to these animals. Trypophobia, the fear of clusters of irregular holes or bumps, is extremely common but is not yet formally classified in the DSM-5. Social phobia (fear of being judged in social situations) affects millions of Indians who struggle with public speaking, networking, or everyday social interactions.
Q3. What is trypophobia?
Trypophobia is an intense discomfort or fear triggered by irregular patterns of closely packed holes, bumps, or circles, such as lotus seed pods, honeycombs, sponges, or certain skin textures. The typical response includes feelings of disgust, revulsion, itching, and anxiety. While extremely common, with studies suggesting up to 16 percent of people experience it, trypophobia is not yet officially listed in the DSM-5. It may represent an evolutionary response to patterns associated with disease or dangerous animals. Trypophobia is generally not treated unless it significantly impairs daily life, in which case gradual desensitisation is effective.
Q4. How are phobias treated?
Specific phobias are among the most treatable mental health conditions. The gold-standard treatment is exposure therapy, in which the person gradually and systematically confronts the feared object or situation in a safe, controlled setting until the fear response diminishes. For simple phobias, even a single intensive session of approximately three hours can produce 80 to 90 percent improvement. CBT helps challenge the irrational beliefs that maintain the phobia. Virtual Reality Exposure Therapy is now available in some Indian clinics for phobias such as flying and heights. Medication (beta-blockers, short-term benzodiazepines) can manage acute situations but does not treat the underlying phobia.
Q5. How many phobias are there?
There is no definitive count. Hundreds of specific fears have been named, with estimates ranging from 400 to over 500. However, the DSM-5 organises specific phobias into five situational categories rather than listing individual named fears. Most named phobias (such as hippopotomonstrosesquippedaliophobia, the fear of long words) are informal coinings rather than formally recognised clinical diagnoses. In practice, any object, situation, or activity can become the focus of a specific phobia if it triggers significant fear and avoidance. The most clinically relevant are those in the top 20 list of common phobias that are routinely treated by mental health professionals.
Q6. Can phobias be cured completely?
Yes. Specific phobias have among the highest treatment success rates of any mental health condition. With exposure therapy, most people experience dramatic and lasting reductions in their phobia, often after just a few sessions. For simple specific phobias, a single extended exposure therapy session produces lasting recovery in 80 to 90 percent of cases. Social phobia typically takes longer, 12 to 20 sessions of CBT, but also has excellent outcomes. The key variable is willingness to engage in exposure: avoiding the feared stimulus maintains the phobia indefinitely, while gradual confrontation significantly reduces it, often to a point where it no longer interferes with life.
Q7. What are some weird or unusual phobias?
Beyond common phobias, many unusual ones have been documented. Nomophobia, the fear of being without a mobile phone, is increasingly prevalent among Indian youth. Ergophobia is the fear of work. Xanthophobia is the fear of the colour yellow. Arithmophobia is the fear of numbers. Ablutophobia is the fear of bathing. Hippopotomonstrosesquippedaliophobia is the ironic fear of long words. Anatidaephobia is the fear that somewhere, a duck is watching you. These unusual phobias, while often discussed with amusement, can be genuinely debilitating for those who experience them. Any specific phobia, regardless of how unusual it seems to others, can be treated effectively with exposure-based therapy.
Additional Resources
- Facing Your Fears Workbook- University of Exeter: https://warwick.ac.uk/services/dc/pgr/phd_wellbeing/facing_your_fears.pdf
- Information on Phobia- Mind : https://www.mind.org.uk/media/7065/phobias-2021.pdf
References
- American Psychiatric Association. (n.d.). What are anxiety disorders? https://www.psychiatry.org/patients-families/anxiety-disorders/what-are-anxiety-disorders
- American Psychological Association. (n.d.). Exposure therapy. https://www.apa.org/ptsd-guideline/patients-and-families/exposure-therapy
- Cleveland Clinic. (n.d.). Aerophobia (fear of flying). https://my.clevelandclinic.org/health/diseases/22431-aerophobia-fear-of-flying
- Cleveland Clinic. (n.d.). Arachnophobia (fear of spiders). https://my.clevelandclinic.org/health/diseases/21852-arachnophobia-fear-of-spiders
- Cleveland Clinic. (n.d.). Amaxophobia (fear of driving). https://my.clevelandclinic.org/health/diseases/22558-amaxophobia-fear-of-driving
- Cleveland Clinic. (n.d.). Cognitive behavioral therapy (CBT). https://my.clevelandclinic.org/health/treatments/21208-cognitive-behavioral-therapy-cbt
- Cleveland Clinic. (n.d.). Cynophobia (fear of dogs). https://my.clevelandclinic.org/health/diseases/22082-cynophobia-fear-of-dogs
- Cleveland Clinic. (n.d.). Phobias. https://my.clevelandclinic.org/health/diseases/24757-phobias
- Cleveland Clinic. (n.d.). Trypanophobia (fear of needles). https://my.clevelandclinic.org/health/diseases/22731-trypanophobia-fear-of-needles
- Cleveland Clinic. (n.d.). Trypophobia. https://my.clevelandclinic.org/health/diseases/21834-trypophobia
- Cleveland Clinic. (n.d.). Vasovagal syncope. https://my.clevelandclinic.org/health/diseases/23325-vasovagal-syncope
- Cleveland Clinic. (n.d.). Tunnel vision (peripheral vision loss). https://my.clevelandclinic.org/health/symptoms/24435-tunnel-vision-peripheral-vision-loss
- Cleveland Clinic. (n.d.). Beta-blockers. https://my.clevelandclinic.org/health/treatments/22318-beta-blockers
- Cleveland Clinic. (n.d.). Benzodiazepines. https://my.clevelandclinic.org/health/treatments/24570-benzodiazepines-benzos
- Harvard Health Publishing. (n.d.). Phobia (A to Z). https://www.health.harvard.edu/a_to_z/phobia-a-to-z
- HelpGuide. (n.d.). Exposure therapy. https://www.helpguide.org/mental-health/treatment/exposure-therapy
- Mayo Clinic. (n.d.). Agoraphobia. https://www.mayoclinic.org/diseases-conditions/agoraphobia/symptoms-causes/syc-20355987
- Mayo Clinic. (n.d.). Depersonalization-derealization disorder. https://www.mayoclinic.org/diseases-conditions/depersonalization-derealization-disorder/symptoms-causes/syc-20352911
- Mayo Clinic. (n.d.). Panic attacks. https://www.mayoclinic.org/diseases-conditions/panic-attacks/symptoms-causes/syc-20376021
- Mayo Clinic. (n.d.). Selective serotonin reuptake inhibitors (SSRIs). https://www.mayoclinic.org/diseases-conditions/depression/in-depth/ssris/art-20044825
- Mayo Clinic. (n.d.). Social anxiety disorder. https://www.mayoclinic.org/diseases-conditions/social-anxiety-disorder/symptoms-causes/syc-20353561
- Mayo Clinic. (n.d.). Specific phobias: Diagnosis and treatment. https://www.mayoclinic.org/diseases-conditions/specific-phobias/diagnosis-treatment/drc-20355162
- Medical News Today. (n.d.). Anticipatory anxiety. https://www.medicalnewstoday.com/articles/anticipatory-anxiety
- Medical News Today. (n.d.). Phobias. https://www.medicalnewstoday.com/articles/320008
- Mental Health America. (n.d.). Phobias. https://mhanational.org/conditions/phobias/
- National Institute of Mental Health and Neurosciences. (2017). National Mental Health Survey of India, 2015–16. https://pmc.ncbi.nlm.nih.gov/articles/PMC5573556/
- Ost, L. G. (1989). One-session treatment for specific phobias. Behaviour Research and Therapy. https://pubmed.ncbi.nlm.nih.gov/2914000/
- Öhman, A., & Mineka, S. (2001). Fears, phobias, and preparedness. Psychological Science. https://journals.sagepub.com/doi/10.1111/1467-8721.01211
- Rachman, S. (1977). The conditioning theory of fear-acquisition. Behaviour Research and Therapy.
- ScienceDirect. (n.d.). Specific phobia research. https://www.sciencedirect.com/science/article/abs/pii/S0887618513000844
- Tele-MANAS. (n.d.). National tele mental health programme of India. https://telemanas.mohfw.gov.in/home
- Verywell Mind. (n.d.). Diagnosing a specific phobia. https://www.verywellmind.com/diagnosing-a-specific-phobia-2671981
- Verywell Mind. (n.d.). Trypophobia. https://www.verywellmind.com/trypophobia-4687678
- Verywell Mind. (n.d.). Nomophobia. https://www.verywellmind.com/nomophobia-the-fear-of-being-without-your-phone-4781725
- Verywell Mind. (n.d.). Xanthophobia. https://www.verywellmind.com/xanthophobia-fear-of-the-color-yellow-7565227
- WebMD. (n.d.). Virtual reality exposure therapy. https://www.webmd.com/anxiety-panic/virtual-reality-exposure-therapy-overview