
.png)

Mental Health Concerns
OCD Full Form, Meaning, Symptoms & Treatment: A Complete Guide (India 2026)
.png)
Written by
Aarohi Parakh,
Psychologist and Content Writer

Reviewed by
Sanjana Sivaram,
Psychologist and Clinical Content Head






Introduction

Priya is a 27-year-old chartered accountant living in Mumbai. She is meticulous, well-regarded, and, to everyone who knows her, hardworking and honest. Every morning before leaving the house, she checks the gas knob fourteen times. She knows, intellectually, that it is off. She checked it for the twelfth time a minute ago. But the doubt comes back, urgent and unrelenting, and she cannot leave until the ritual is complete. On bad days, she is forty minutes late for work.
She has never told anyone. She assumes it is anxiety, or perhaps that she is simply someone who needs to be thorough at all times. It has not occurred to her that what she is living with has a name, a diagnosis, and evidence-based treatments that help a significant proportion of people experience meaningful symptom reduction and improved functioning, with research showing response rates of approximately 40-60 percent depending on severity and treatment approach.
Priya is living with OCD. And she is far from alone. OCD affects an estimated 2 to 3.3 percent of people in India, making it one of the more common serious mental health conditions in the country. It is also one of the most misunderstood, most frequently joked about, and most inadequately treated. This guide covers everything you need to know: the full form and meaning of OCD, its types, symptoms, causes, and evidence-based treatment options available in India.
OCD Full Form and Meaning: What Does OCD Stand For?
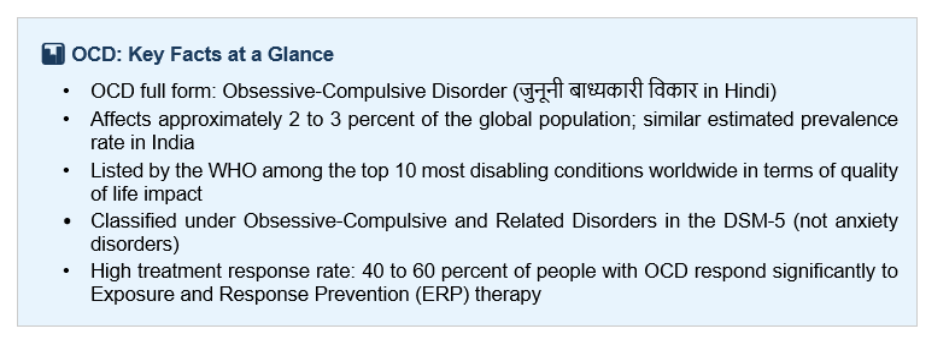
OCD full form: Obsessive-Compulsive Disorder. In medical terminology, it falls under the category of Obsessive-Compulsive and Related Disorders in the DSM-5 TR (Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition), published by the American Psychiatric Association. It is classified not as an anxiety disorder (despite anxiety being central to it), but in the category that also includes body dysmorphic disorder, hoarding disorder, and trichotillomania.
OCD full form in Hindi: जुनूनी बाध्यकारी विकार (Junooni Badhyakari Vikar). OCD kya hota hai? Yeh ek aisi mansik sthiti hai jisme baar-baar aane wale anichche vichaar (obsessions) aur unhe door karne ke liye ki jaane wali baar-baar ki kriyaayein (compulsions) hoti hain.
OCD meaning in Tamil: அக்கினை-கட்டாயப் பிறழ்வு (Akkinai-Kattayap Pirazhvu) — the Tamil clinical equivalent used in psychiatric settings across Tamil Nadu.
A critical clarification: OCD is not a personality trait. Saying 'I'm so OCD about my desk' trivialises a serious and often debilitating condition. OCD involves intrusive, unwanted thoughts that feel impossible to dismiss, and compulsions that are not experienced as pleasurable but as necessary to prevent something terrible from happening. It consumes time, causes significant distress, and impairs the ability to function.
What Is OCD? Understanding the Condition
OCD is a mental health condition characterised by two interlocking components: obsessions and compulsions.
Obsessions are repetitive, intrusive thoughts, images, or urges that enter a person’s mind without intention and cause significant distress. They are ego-dystonic, meaning they go against the person’s values and desires, which is why they feel disturbing. For example, in harm OCD, the individual has no wish to hurt anyone. The distress comes from the very presence of these unwanted thoughts.
Compulsions are repetitive behaviours or mental acts performed in response to an obsession, with the goal of reducing anxiety or preventing a feared outcome. Compulsions provide only temporary relief. The obsession returns, often more intensely, and the compulsion must be performed again. This reinforcing cycle is what makes OCD self-sustaining and, without treatment, progressive.
To meet the diagnostic threshold for OCD, obsessions and compulsions must consume more than one hour per day and cause significant distress or impairment. At its most severe, OCD can consume the majority of a person's waking life. The WHO ranks OCD among the top 10 most disabling conditions in the world in terms of loss of income and quality of life.
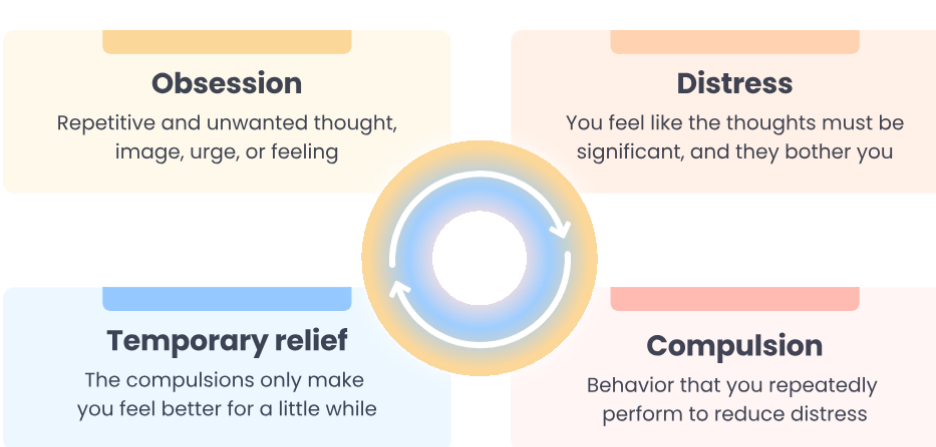
The cycle above is self-reinforcing: each compulsion provides temporary relief that reinforces the belief that the obsession is genuinely dangerous, making the next obsessional episode more powerful. Breaking the cycle requires resisting the compulsion, the core mechanism of ERP therapy.
OCD affects people across all demographics in India. It appears in children, teenagers, working adults, and the elderly. It presents across all economic classes, educational backgrounds, and geographies. With a prevalence rate of 2 to 3.3 percent in India, the condition continues to remain significantly underdiagnosed because it is frequently mistaken for religiosity, excessive diligence, or anxiety, particularly in settings where mental health literacy is limited.
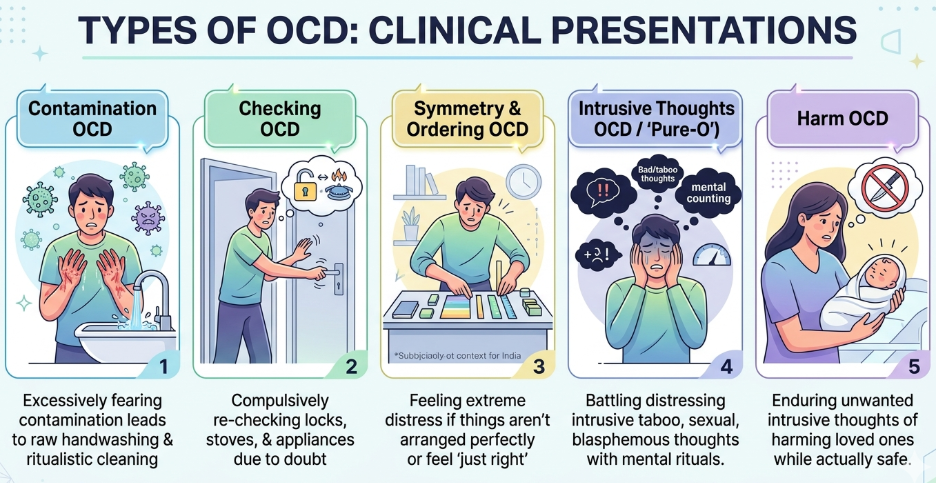
What Are the Types of OCD?
The question 'what are the types of OCD?' reflects how clinicians and researchers commonly categorise OCD presentations for treatment planning. While the DSM-5 TR does not formally divide OCD into subtypes, clinical literature identifies the below presentations.
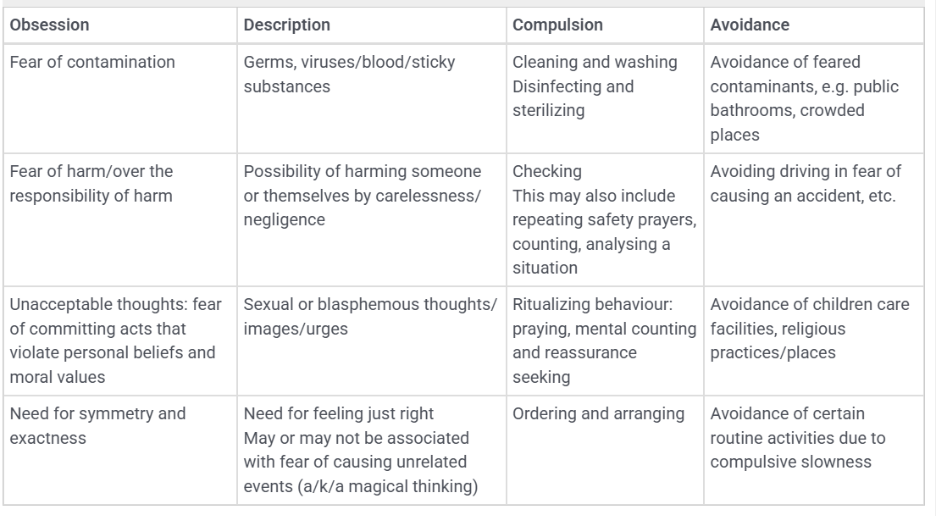
1. Contamination OCD
Contamination OCD is one of the most recognisable presentations and among the most prevalent in India, where concerns about purity, ritual cleanliness, and pollution carry significant cultural weight. The obsessional content centres on fear of germs, illness, dirt, or contamination, either from external sources such as surfaces, public places, or other people, or from internal sources such as bodily fluids or certain foods.
Compulsions: Excessive handwashing (which can reach 50 to 100 times per day until skin is raw and bleeding), showering rituals that last hours, avoiding 'contaminated' surfaces, discarding items that have been touched, and seeking repeated reassurance that one has not been contaminated.
India context: In Indian households, where ritual cleanliness (shuddhi) before prayer and after toileting is culturally embedded, contamination OCD can be extremely difficult to identify because its compulsions mirror normalised practices. The clinical indicator is always disproportionality and impairment.
2. Checking OCD
Checking OCD is characterised by persistent doubt and an exaggerated sense of responsibility about preventing harm or avoiding disaster. The core obsession revolves around uncertainty, such as “What if I made a mistake?” or “What if something bad happens because of me?” Even after a task is completed, the person struggles to trust their memory or perception, leading to repeated checking.
Compulsions: Repeatedly checking locks, gas stoves, switches, appliances, and doors; going back multiple times to confirm safety; re-reading messages or emails to ensure no error was made; repeatedly reviewing actions in one’s mind; and seeking reassurance from others that everything is safe or correct. Checking can consume hours of the day without bringing lasting relief.
India context: In Indian households, where safety concerns around gas leaks, electrical appliances, and home security are common, checking behaviours may initially appear practical or responsible. However, in Checking OCD, the behaviour becomes excessive, time-consuming, and distress-driven rather than precautionary. Individuals may be labelled as “overthinkers” or “too careful,” which delays recognition and treatment.
3. Symmetry and Ordering OCD
Symmetry and ordering OCD involves a need for objects, actions, or situations to feel 'just right', often described as an uncomfortable sense of incompleteness or asymmetry that persists until corrected. Unlike a preference for tidiness, this need causes significant distress when it cannot be satisfied, and the associated compulsions can be time-consuming.
Compulsions: Arranging objects until they feel 'right', repeating actions a specific number of times, counting, tapping, touching objects in a particular sequence, and re-reading or re-writing until it feels correct.
India context: This presentation is often highly visible but is frequently attributed to personality traits such as perfectionism. In Indian academic settings, where precision and order are socially valued, symmetry OCD can be inadvertently reinforced by family and teachers as evidence of good character.
4. Intrusive Thoughts OCD (Pure-O)
Sometimes called 'Pure-O' (for pure obsessional), this presentation is characterised by distressing intrusive thoughts of a taboo nature, including thoughts that are sexual, violent, blasphemous, or morally intolerable. The name 'Pure-O' is somewhat misleading: compulsions are always present, but they are mental in nature rather than behavioural, involving rumination, mental review, neutralising thoughts, and compulsive reassurance-seeking.
Compulsions: Mental rituals (replacing a 'bad' thought with a 'good' one), rumination, confessing thoughts to others to seek reassurance, praying to counteract 'sinful' thoughts, and compulsive avoidance of situations that might trigger the thoughts.
India context: Religious or scrupulosity OCD is a highly prevalent presentation in India across Hindu, Muslim, Sikh, and Christian communities. It involves intrusive blasphemous thoughts, fear of having sinned, excessive prayer performed not as devotion but as anxiety reduction, and confession rituals. It is among the least recognised and most undertreated presentations of OCD in India, because the compulsions are often indistinguishable from religious practice without a careful clinical assessment.
5. Harm OCD
Harm OCD involves recurrent, intrusive thoughts about accidentally or deliberately harming oneself or others. It is essential to understand that people with harm OCD do not want to act on these thoughts. The thoughts are profoundly unwanted and ego-dystonic, which is precisely why they cause such distress. A loving parent who has intrusive thoughts about harming their newborn is not a danger; they are experiencing a very common OCD presentation.
Compulsions: Checking behaviours (for signs of injury or evidence of wrongdoing), hiding or removing sharp objects, avoiding situations where harm feels possible, seeking constant reassurance from others, praying or repeating phrases to “cancel” bad thoughts, and mental review of past actions to confirm no harm has been done.
India context: Harm OCD is among the presentations most likely to go undiagnosed in India because the person, ashamed of the intrusive thoughts, conceals them entirely. The shame and secrecy around these thoughts are a hallmark of their ego-dystonic nature, and they should always be distinguished from genuine intent to harm, which is categorically different.
⚠️ Critical Clarification: Harm OCD and Safety
- People with Harm OCD are not dangerous. The intrusive thoughts that characterise Harm OCD are ego-dystonic: deeply unwanted, distressing, and actively resisted.
- Genuine violent intent is ego-syntonic: the person wants to act. In Harm OCD, the opposite is true.
Misidentifying Harm OCD as dangerous is a common and harmful error. If you or someone you know is experiencing intrusive thoughts of harm, please seek assessment from a qualified mental health professional rather than assuming risk.
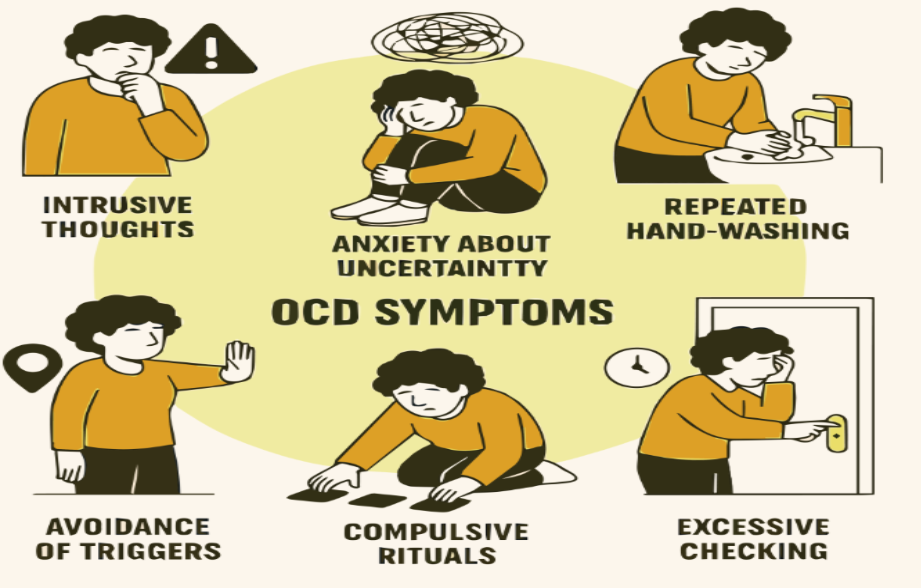
OCD Symptoms: How to Identify Obsessions and Compulsions
OCD symptoms (OCD ke lakshan) span both obsessional content and compulsive behaviour, and they vary considerably across individuals. The following is a structured overview of common presentations.
Common Obsessions
- Fear of contamination from germs, dirt, illness, or bodily fluids
- Fear of accidentally harming oneself or others, or of having already done so
- Need for objects or actions to be symmetrical or 'just right'
- Intrusive sexual, violent, or blasphemous thoughts that feel deeply disturbing
- Fear of making a mistake with serious consequences (leaving the gas on, causing an accident)
- Scrupulosity: fear of sinning, offending a deity, or being morally corrupt
Common Compulsions
- Handwashing: can reach 50 to 100 times per day; may continue until hands bleed
- Checking: locks, gas knobs, switches, or the safety of loved ones; returning home multiple times to verify
- Counting, tapping, or repeating actions a specific number of times
- Arranging objects until they feel symmetrical or correct
- Mental rituals: replacing 'bad' thoughts with 'good' ones, mentally reviewing past actions, praying as anxiety reduction
- Seeking reassurance from family members that nothing bad has happened
- Avoiding situations, objects, or people associated with obsessional fears
OCD Symptoms in Hindi (OCD ke Mukhya Lakshan)
Obsessions (Junooni Vichaar): bar-bar aane wale anichche vichaar jaise gandagi ka darr, doosron ko nuksan pahunchane ka bhay, ya dharmik paap ka darr.
Compulsions (Badhyakari Kriyaayein): baar-baar haath dhona, baar-baar taale ya gas ka check karna, cheezein baar-baar seedhi karna ya ginana.

Could I Have OCD? A Self-Check
The Yale-Brown Obsessive Compulsive Scale (Y-BOCS) is the gold-standard clinical assessment tool for OCD severity. The following questions are adapted from validated screening tools and are not a substitute for clinical diagnosis:
- Do you have recurring thoughts, images, or urges that feel intrusive and unwanted?
- Do these thoughts cause you significant anxiety or distress?
- Do you perform repetitive behaviours or mental rituals to reduce that anxiety?
- Do these thoughts and behaviours consume more than one hour of your day?
- Do they interfere with your work, relationships, or daily functioning?
If you answered yes to three or more of these questions, it is worth speaking to a mental health professional for a formal assessment.
If you or someone you know is struggling, help is available:
- Access confidential counselling through Employee Assistance Programme (EAP) providers such as 1to1help (check with your HR on enrolled EAP services)
- For immediate support, contact Tele MANAS 14416 (free, 24/7, multiple Indian languages)
- Depending on the severity and frequency of your symptoms, working with a trained psychologist or psychiatrist can provide structured, evidence-based treatment.
What Causes OCD? Risk Factors and Triggers
OCD does not have a single cause. Like most mental health conditions, it develops through the interaction of biological vulnerability, psychological patterns, and environmental triggers. Understanding these factors reduces the blame and shame that many people with OCD in India carry.
Biological Factors
OCD has a strong genetic component. Research suggests a heritability rate of 40 to 50 percent, meaning that biological predisposition plays a significant role.
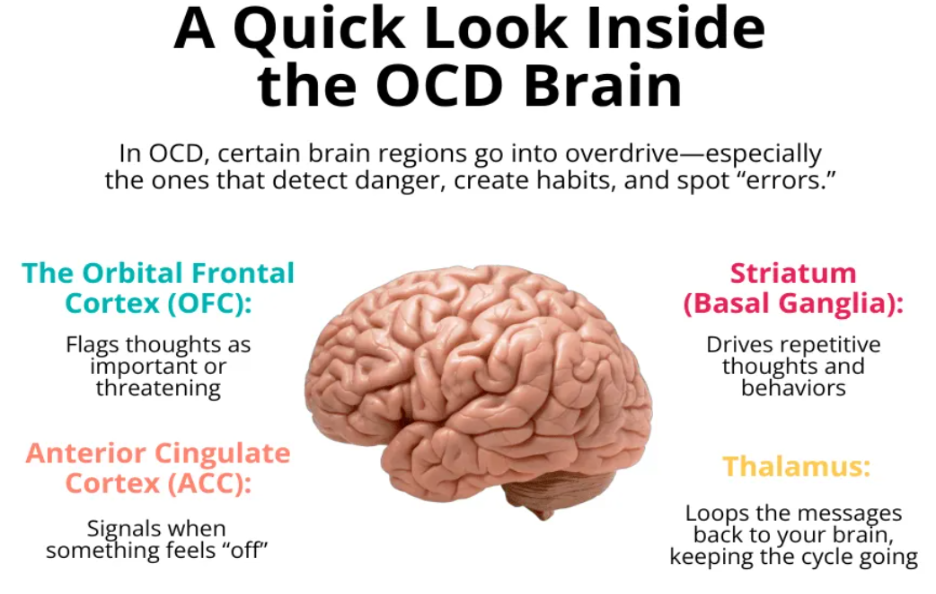
Neuroimaging studies and research shows that OCD is linked to certain parts of the brain, including the orbitofrontal cortex (OFC), anterior cingulate cortex (ACC), thalamus, and basal ganglia.
In simple terms, these areas have different roles:
- The OFC helps shape our thoughts, emotions, and gut feelings
- The ACC helps us notice mistakes and stay alert
- The thalamus acts like a relay system, sending signals related to movement and sensations
- The basal ganglia help us plan and carry out actions
People with OCD have what researchers sometimes describe as an overactive 'danger alarm': the brain generates a sense of threat that persists even after rational reassessment.
At a neurochemical level, dysregulation in serotonin and, more recently identified, glutamate pathways contribute to OCD. This is why SSRIs, which act on serotonin, are an effective pharmacological treatment. Research has also shown that differences in the neurotransmitters dopamine and GABA can also contribute to the progression of OCD.
Psychological Factors
Certain cognitive patterns are strongly associated with OCD: perfectionism (the belief that mistakes are catastrophic), thought-action fusion (the belief that having a thought is equivalent to intending it), inflated responsibility (the belief that one must prevent all possible harm), and intolerance of uncertainty. These appraisal styles are the targets of the cognitive component of CBT for OCD.
Environmental Triggers in India
- Streptococcal infections (PANDAS): Paediatric Autoimmune Neuropsychiatric Disorders Associated with Streptococcal Infections (PANDAS) cause sudden-onset OCD in children following a streptococcal throat infection. This mechanism is under-recognised in Indian paediatric settings, where an abrupt onset of rituals or tics following a throat infection should prompt evaluation for PANDAS.
- High-stakes examinations: The intense pressure of board exams, JEE, NEET, and UPSC preparation creates conditions in which checking, symmetry, and perfectionism-driven compulsions can emerge or worsen. Academic environments that reward absolute precision can inadvertently amplify OCD-prone cognitive styles.
- Life transitions: Marriage, childbirth, moving cities for work, and bereavement are common OCD trigger events in India. The onset of postpartum OCD, in which new mothers experience intrusive thoughts about harming their infant, is significantly underidentified and undertreated in Indian healthcare settings.
- Religious and cultural amplifiers: India's rich tradition of ritual practice, while generally protective for wellbeing, can provide the structure through which scrupulosity OCD expresses itself. Compulsive prayer, excessive purification rituals, and the inability to complete religious practice without starting again from the beginning are common presentations that are frequently attributed to piety rather than recognised as OCD.
OCD Treatment: Therapy, Medication, and Recovery in India
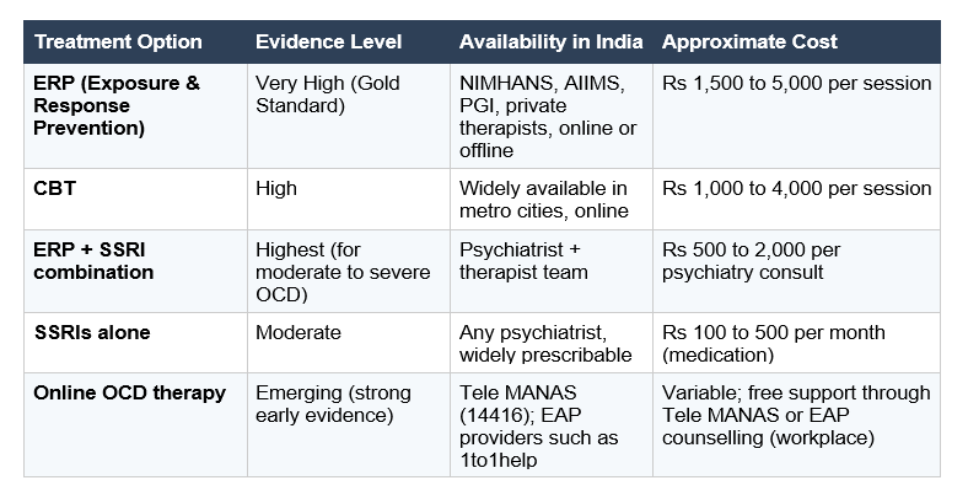
OCD treatment in India has improved significantly over the past decade, and the prognosis with proper treatment is genuinely hopeful. The IOCDF reports that on average, a 60 percent reduction in OCD symptoms is achieved with Exposure and Response Prevention therapy, the gold-standard treatment.
Exposure and Response Prevention (ERP): The Gold Standard
ERP is the most effective psychological treatment for OCD, with decades of robust evidence behind it. Developed by Joseph Wolpe and later refined by Edna Foa and the International OCD Foundation (IOCDF), ERP works by exposing the person to situations or stimuli that trigger obsessional anxiety, while preventing the compulsive response. Over time, and through a process called habituation, the anxiety diminishes without the compulsion.
How it works: The therapist and client collaboratively build a fear hierarchy: a ranked list of feared triggers from least to most anxiety-provoking. The client begins exposure with lower-level items, learns that the anxiety passes without the compulsion, and progressively works up the hierarchy. For Priya, from our opening, this might begin with touching a door handle without immediately washing her hands, staying with the discomfort, gradually learning that the anxiety naturally reduces even without performing the compulsion. Over time, it can be extended to her other triggers, such as touching the office desk or travelling in local trains.
ERP is not comfortable. It requires courage, commitment, and a skilled therapist who understands OCD. But it produces lasting change in a way that avoidance and reassurance-seeking cannot.
Cognitive Behavioural Therapy (CBT)
CBT focuses on the thought patterns that maintain OCD, such as:
- “If I think it, it might happen” (thought-action fusion)
- “I must be 100 percent certain”
- “If something goes wrong, it will be my fault”
Case example: Rohan, a college student, experienced intrusive harm thoughts and believed that having the thought meant he was dangerous. Through CBT, he learned that thoughts are not actions. This reduced his fear and helped him engage better in ERP exercises.
CBT is most effective when combined with ERP, not used alone. For social anxiety co-occurring with OCD, CBT addresses both simultaneously.
Medication: SSRIs for OCD
SSRIs (Selective Serotonin Reuptake Inhibitors) are the first-line pharmacological treatment for OCD. The SSRIs with the strongest evidence base for OCD include Fluvoxamine, Sertraline, and Fluoxetine.
A critical point: OCD typically requires higher doses of SSRIs than depression, and the full therapeutic effect takes 6 to 12 weeks to manifest. Starting at a low dose and expecting rapid results is a common treatment error.
Case example: Meena, a 40-year-old homemaker, had severe checking OCD and was unable to leave the house. Medication helped reduce her baseline anxiety, making it possible for her to engage in ERP and gradually regain independence.
For moderate to severe OCD, the combination of ERP with an SSRI is the most effective approach. Medication alone, without ERP, rarely produces lasting recovery because it does not address the underlying behavioural cycle.
Treatment Options in India: A Quick Reference
Recovery: What to Expect
Recovery from OCD is realistic. Most people with OCD who engage with proper treatment, particularly ERP, experience a significant reduction in symptoms. Some achieve long-term remission. Recovery from OCD does not mean “no intrusive thoughts.” It means:
- Thoughts no longer control behaviour
- Compulsions reduce significantly
- Daily functioning improves
Case example: Aman, a 32-year-old IT professional, continued to have occasional intrusive thoughts even after therapy. The difference was that he no longer engaged with them. He returned to work, travel, and social life without being dominated by OCD.
Relapse can happen, especially during stress. However, individuals who have learned ERP skills are better equipped to manage it independently or with brief support.
💡Clinical Insight: The biggest shift in OCD recovery is not symptom elimination, but building tolerance for uncertainty. This is why ERP works where reassurance and avoidance fail.
OCD in Children and Teenagers in India
OCD often begins in childhood, adolescence, or early adulthood. Research suggests the average age of onset is around 19 years (25% cases begin by age 14), with many individuals reporting that symptoms started much earlier but went unrecognised for years. In India, two factors specifically shape childhood OCD: the high-pressure academic environment and the tendency of families to accommodate compulsions unknowingly.
How Childhood OCD Presents Differently
- School refusal driven by contamination fears or symmetry distress
- Bedtime rituals that must be performed in a precise order before sleep is possible
- Repeated, reassurance-seeking questions to parents ('Are you sure it is safe?')
- Difficulty completing schoolwork due to erasing and rewriting until 'perfect'
- Avoidance of certain topics, objects, or places without apparent reason
- Suddenly excessive prayer or religious ritual following normal participation
Academic pressure as a trigger: The intense competition around board exams, JEE, NEET, and other entrance examinations creates ideal conditions for the emergence or worsening of checking and perfectionism-driven OCD. Students who begin rewriting notes compulsively, checking their answers repeatedly, or feeling paralysed by the need to get everything exactly right may be showing early signs of OCD rather than diligence. Understanding this distinction, rather than praising the behavior as an admirable work ethic, can significantly accelerate appropriate support.
Family Accommodation and Children
Family accommodation in childhood OCD is a significant clinical concern. When parents wash items repeatedly because their child insists, provide frequent reassurance, or avoid certain situations to reduce the child’s distress, they may unintentionally reinforce the OCD cycle. Research shows that family accommodation is associated with greater symptom severity and can interfere with treatment progress. For this reason, involving parents in treatment is essential. Family-based approaches help reduce accommodation while supporting the child in facing anxiety more effectively.
💡 Guidance for Parents of Children with OCD
- Do not participate in rituals or provide repeated reassurance. It feels unkind in the moment but maintains the OCD.
- Do not force confrontation with feared stimuli. ERP must be gradual and therapist-guided.
- Approach the child's distress with empathy rather than frustration. The child is not being difficult; they are experiencing genuine anguish.
- Seek assessment from a child psychiatrist or psychologist trained in OCD, not a general paediatric appointment.
Consider whether academic pressure is a trigger. A conversation with the school about reducing performance expectations during treatment may be warranted.
OCD in the Indian Workplace
OCD in working adults is among the most consequential and least addressed mental health presentations in Indian organisations. It is also, for reasons of stigma and concealment, among the hardest to identify. Employees with OCD are often high-performers on the surface, with a reputation for thoroughness and precision, while managing an exhausting private reality of rituals, checking, and intrusive thoughts. Many professionals do not initially recognise these patterns as OCD because behaviours such as meticulousness, overchecking, perfectionism, and excessive responsibility are often praised in Indian workplaces as signs of dedication, reliability, or strong work ethic.
Common occupational impacts of OCD include:
- Spending several additional hours checking work before submitting, causing consistent overruns
- Arriving late due to morning rituals (checking locks, washing, dressing rituals that cannot be interrupted)
- Difficulty making decisions due to fear of making an irreversible mistake
- Avoiding professional feedback or appraisal due to the anxiety triggered by external scrutiny
- Reduced output due to the mental bandwidth consumed by obsessional thought
- Presenteeism: appearing functional while managing severe internal distress
EAP (Employee Assistance Programme) counselling through providers such as 1to1help offers a confidential, accessible first point of contact for employees who suspect they may have OCD. EAP services can provide initial assessment, psychoeducation, and referral to specialist treatment. For managers, the most important response to a team member with suspected OCD is empathy and guiding them to support, rather than performance management.
📊 OCD and Attrition: The Hidden Cost
- Untreated OCD significantly increases the risk of employee attrition. The combination of daily exhaustion, performance anxiety, and the absence of support creates conditions for disengagement and quiet quitting.
- OCD is estimated to cause an average of 46 working days of lost productivity per person per year in untreated cases.
Early identification and access to ERP-trained therapy can significantly reverse this trajectory. EAP counselling is the most accessible entry point for employed adults in India.
A Final Word
OCD is not a quirk. It is not a punchline. And it is not a life sentence. Priya, the accountant from our opening, eventually spoke to a therapist through her company's EAP. She was assessed, diagnosed, and referred to an ERP-trained psychologist. Twelve weeks into treatment, she was leaving the house in the morning without checking the gas knob. She described it, tentatively, as feeling like someone had turned the volume down.
That is what proper treatment does. It does not eliminate the experience of life; it returns the person to it.
If something in this guide feels familiar, consider reaching out. You can start with the Government of India’s Tele MANAS helpline at 14416 for free, immediate support. If your workplace offers Employee Assistance Programme services such as those provided by 1to1help, these can be a confidential and accessible first step. Depending on the severity and frequency of your symptoms, working with a trained psychologist or psychiatrist can provide structured, evidence-based treatment.
You do not have to wait for it to get worse to take it seriously.
Understanding what is happening is the first step. Acting on it is the next.
FAQs
Q1. What is the full form of OCD?
OCD stands for Obsessive-Compulsive Disorder. In medical terminology, it is classified under Obsessive-Compulsive and Related Disorders in the DSM-5 TR, the diagnostic manual of the American Psychiatric Association. In Hindi, the OCD full form in Hindi is जुनूनी बाध्यकारी विकार (Junooni Badhyakari Vikar). In medical settings across India, the English acronym OCD is universally used. OCD affects approximately 2 to 3 percent of the global population, and similar estimates are prevalent in India. It is a diagnosable and treatable mental health condition, not a personality trait.
Q2. What are the different types of OCD?
OCD generally presents in below mentioned main types: 1) Contamination OCD involves fear of germs or illness, with compulsive cleaning or handwashing. 2) Checking OCD involves constant doubt and a strong need to prevent harm, making a person repeatedly check things even after completing them. They struggle to trust their memory, so they continue checking despite knowing it was already done. 3) Symmetry and Ordering OCD involves a need for things to be 'just right', with arranging, counting, and repeating compulsions. 4) Intrusive Thoughts OCD (Pure-O) involves disturbing thoughts of a taboo nature, managed through mental rituals. 5) Harm OCD involves intrusive, unwanted thoughts of accidentally or deliberately harming others, managed through checking and reassurance-seeking. It is important to note that people with Harm OCD do not want to act on their thoughts. The intrusive thoughts in all types are ego-dystonic: deeply unwanted and distressing.
Q3. Is OCD curable?
OCD is not always fully 'cured', but it is highly treatable and manageable. With the right treatment, particularly Exposure and Response Prevention (ERP) therapy and SSRIs, most people with OCD experience a significant reduction in symptoms and a greatly improved quality of life. Some achieve long-term remission, in which symptoms rarely interfere with daily functioning. In India, access to trained ERP therapists is growing through specialist centres such as NIMHANS, AIIMS, and online therapy platforms. The key is finding a therapist with specific OCD expertise: not all CBT therapists are trained in ERP.
Q4. What is the difference between OCD and being a clean freak?
This is one of the most common misconceptions about OCD. Being particular about cleanliness or order is a personality preference and does not cause significant distress or impairment. OCD, by contrast, is driven by intrusive, unwanted thoughts that feel impossible to dismiss, and the compulsions performed to relieve them are distressing, time-consuming, and significantly interfere with daily life. A person with contamination OCD may wash their hands 50 to 100 times a day until the skin is cracked and bleeding, not because they enjoy cleanliness, but because they cannot stop without experiencing overwhelming anxiety. OCD is a diagnosable mental health condition, not a personality trait or a preference.
Q5. How is OCD treated in India?
The most effective treatment for OCD in India is Exposure and Response Prevention (ERP) therapy, a specialised form of CBT. SSRIs such as Fluvoxamine and Sertraline are also effective, particularly for moderate to severe OCD, and are available through psychiatrists across India. Specialists are available at NIMHANS Bangalore, AIIMS Delhi, and PGI Chandigarh. Online/offline OCD therapy is increasingly available through different practising therapists. The Tele MANAS helpline (14416) can provide initial guidance. ERP combined with medication is the most effective combination for moderate to severe OCD. Employees can access initial support confidentially through EAP counselling.
Q6. Can OCD affect children in India?
Yes. OCD often first appears in childhood or adolescence, with a mean onset age of 19. In India, the high-pressure academic environment, particularly around board exams and entrance tests such as JEE and NEET, can trigger or significantly worsen OCD. Childhood OCD may look different from adult presentations: school refusal, insistence on bedtime rituals, constant reassurance-seeking from parents, and compulsive erasing and rewriting. Indian families often unknowingly worsen OCD by participating in or accommodating the child's rituals. Child-specific ERP therapy, family therapy, and school support are effective. If you suspect your child has OCD, seek assessment from a child psychiatrist rather than attributing the behaviour to diligence or anxiety alone.
Q7. Is OCD a serious mental illness?
Yes. OCD is a serious mental health condition. At its most severe, it can consume several hours a day and prevent a person from working, studying, maintaining relationships, or carrying out basic activities. The WHO lists OCD among the top 10 most disabling conditions worldwide in terms of loss of income and quality of life. In India, OCD is frequently underdiagnosed because many people mistake their symptoms for religious devotion, thoroughness, or anxiety. Early diagnosis and treatment with ERP significantly improve outcomes and prevent the condition from becoming chronic. Seeking help is not a weakness; it is the most rational response to a real condition with highly effective treatment.
Recommended Reading
References
- American Psychiatric Association. (n.d.). Rumination: A cycle of negative thinking. Retrieved from https://www.psychiatry.org/news-room/apa-blogs/rumination-a-cycle-of-negative-thinking
- BrainsWay. (n.d.). Is OCD curable? Retrieved from https://www.brainsway.com/knowledge-center/is-ocd-curable/
- Cleveland Clinic. (n.d.). Basal ganglia. Retrieved from https://my.clevelandclinic.org/health/body/23962-basal-ganglia
- Cleveland Clinic. (n.d.). Dopamine. Retrieved from https://my.clevelandclinic.org/health/articles/22581-dopamine
- Cleveland Clinic. (n.d.). Gamma-aminobutyric acid (GABA). Retrieved from https://my.clevelandclinic.org/health/articles/22857-gamma-aminobutyric-acid-gaba
- Cleveland Clinic. (n.d.). Serotonin. Retrieved from https://my.clevelandclinic.org/health/articles/22572-serotonin
- Cleveland Clinic. (n.d.). Thalamus. Retrieved from https://my.clevelandclinic.org/health/body/22652-thalamus
- Cleveland Clinic. (n.d.). Glutamate. Retrieved from https://my.clevelandclinic.org/health/articles/22839-glutamate
- Healthline. (n.d.). Severe OCD. Retrieved from https://www.healthline.com/health/mental-health/severe-ocd
- Holly Hill Hospital. (n.d.). What are the 4 types of OCD? Retrieved from https://hollyhillhospital.com/blog/what-are-the-4-types-of-ocd-how-to-spot-the-signs/
- International OCD Foundation. (n.d.). What causes OCD? Retrieved from https://iocdf.org/about-ocd/what-causes-ocd/
- International OCD Foundation. (2014). Postpartum OCD fact sheet. Retrieved from https://iocdf.org/wp-content/uploads/2014/10/Postpartum-OCD-Fact-Sheet.pdf
- International OCD Foundation. (n.d.). Exposure and response prevention (ERP). Retrieved from https://iocdf.org/ocd-treatment-guide/exposure-response-prevention/
- Investopedia. (n.d.). Presenteeism. Retrieved from https://www.investopedia.com/terms/p/presenteeism.asp
- JAMA Psychiatry. (2024). [Article on OCD neurobiology]. Retrieved from https://jamanetwork.com/journals/jamapsychiatry/fullarticle/2817090
- Journal of Neuroscience and Psychiatry. (2011). [OCD-related neurocircuitry]. Retrieved from https://psychiatryonline.org/doi/10.1176/jnp.23.2.jnp121
- Mayo Clinic. (n.d.). Body dysmorphic disorder. Retrieved from https://www.mayoclinic.org/diseases-conditions/body-dysmorphic-disorder/symptoms-causes/syc-20353938
- Mayo Clinic. (n.d.). Hoarding disorder. Retrieved from https://www.mayoclinic.org/diseases-conditions/hoarding-disorder/symptoms-causes/syc-20356056
- Mayo Clinic. (n.d.). Obsessive-compulsive disorder (OCD). Retrieved from https://www.mayoclinic.org/diseases-conditions/obsessive-compulsive-disorder/symptoms-causes/syc-20354432
- Mayo Clinic. (n.d.). Selective serotonin reuptake inhibitors (SSRIs). Retrieved from https://www.mayoclinic.org/diseases-conditions/depression/in-depth/ssris/art-20044825
- Mayo Clinic. (n.d.). Social anxiety disorder. Retrieved from https://www.mayoclinic.org/diseases-conditions/social-anxiety-disorder/symptoms-causes/syc-20353561
- Mayo Clinic. (n.d.). Trichotillomania. Retrieved from https://www.mayoclinic.org/diseases-conditions/trichotillomania/symptoms-causes/syc-20355188
- Merriam-Webster. (n.d.). Blasphemous. Retrieved from https://www.merriam-webster.com/dictionary/blasphemous
- MindVoyage. (n.d.). The prevalence of OCD in India. Retrieved from https://mindvoyage.in/the-prevalence-of-ocd-in-india/
- MCPAP. (n.d.). Y-BOCS scale. Retrieved from https://www.mcpap.com/pdf/YBOCS.pdf
- National Medical Journal of India. (n.d.). Diagnosis and treatment of OCD. Retrieved from https://nmji.in/diagnosis-and-treatment-of-obsessivecompulsive-disorder/
- Neuroscientifically Challenged. (n.d.). Orbitofrontal cortex. Retrieved from https://neuroscientificallychallenged.com/posts/know-your-brain-orbitofrontal-cortex
- OCD UK. (n.d.). World Health Organization and OCD. Retrieved from https://www.ocduk.org/ocd/world-health-organisation/
- PubMed. (2012). SSRI treatment outcomes in OCD. Retrieved from https://pubmed.ncbi.nlm.nih.gov/22288678/
- ResearchGate. (2011). Overview of Indian research in OCD. Retrieved from https://www.researchgate.net/publication/51566681_An_overview_of_Indian_research_in_obsessive_compulsive_disorder
- ScienceDirect. (2018). [OCD neurobiology review]. Retrieved from https://pmc.ncbi.nlm.nih.gov/articles/PMC6209853/
- Springer / PMC. (2021). Pharmacological treatment of OCD. Retrieved from https://pmc.ncbi.nlm.nih.gov/articles/PMC8269156/
- Treat My OCD. (n.d.). Ego-dystonic thoughts. Retrieved from https://www.treatmyocd.com/what-is-ocd/info/ocd-stats-and-science/what-are-ego-dystonic-thoughts-how-experts-use-the-term
- Treat My OCD. (n.d.). Harm OCD guide. Retrieved from https://www.treatmyocd.com/blog/what-is-harm-ocd-guide-to-ocd-subtype
- Treat My OCD. (n.d.). Hyper-responsibility OCD. Retrieved from https://www.treatmyocd.com/blog/hyper-responsibility-ocd
- Verywell Mind. (n.d.). Thought-action fusion and OCD. Retrieved from https://www.verywellmind.com/thought-action-fusion-and-ocd-2510478
- Verywell Mind. (n.d.). Bereavement. Retrieved from https://www.verywellmind.com/bereavement-definition-symptoms-causes-traits-treatment-5197038
- World Health Organization (via OCD UK). (n.d.). OCD global impact. Retrieved from https://www.ocduk.org/ocd/world-health-organisation/